


Neonatal intensive care units can be noisy places which can disturb the sleep patterns of the youngest patients in the hospitals and have a negative effect on their health. In an effort to ameliorate this, some NICUs have set quiet times to limit exposure to noise. However, little was known about the effects of the ‘quiet time’ on infant health and it is only now according to a recent study in The Journal of the Acoustical Society of America that researchers have demonstrated its beneficial effect. The study, one of the first in this field, examined the effects of quiet time implementation in multiple NICUs on infants up to 18 months after implementation. They analysed how each NICU’s soundscape changed throughout the day and how this affected infant heart rates. They found that certain stressful pitches were actually quieter in respect to their effect on infant heart rates and that very loud sounds occurred less frequently with the result that quiet time throughout the day was longer. The results provide a sense of which features of quiet time policies have the largest impact on infants in NICUs and they recommend using quiet time protocols to help NICU patients in addition to implementing architectural noise reduction strategies in NICUs.
In a separate, but related study published in Sleep last year, researchers showed that preterm newborns sleep better in NICUs while hearing their mother’s voice. The study explored the possibility that infants’ exposure to their mother’s voice in the NICU could modulate the impact of noise in the NICU. The results indicate that newborns in a NICU were less likely to be awakened by noises when a recording of their mother’s voice was playing. The study also found that newborns born at or after 35 weeks’ gestation show sleep-wake patterns that appear to respond increasingly with age to recorded maternal voice exposure. Similar associations were not found for infants born before 35 weeks’ gestation. It appears that exposure to a mother’s voice recording may insulate NICU patients from some of the impact of unavoidable noise by reducing the likelihood of wakefulness during the highest peak noise levels. Because of this, the researchers suggest that for infants who are ill or born prematurely and may require extended care in a NICU during a time of critical brain development, interventions designed to improve sleep may need to be tailored according to gestational age. As such, the impact of playing a recording of a mother’s voice, reading a story for example, may have a more significant impact for newborns who are near term gestation than for more premature infants.

In February last year, the US Food and Drug Administration (FDA) cleared the first medical device which uses artificial intelligence (AI) to provide clinical decision support for stroke. The Viz.AI Contact application uses an AI algorithm to identify a suspected stroke and notifies a specialist more quickly than was previously possible. Faster treatment, in turn, lessens the extent of a stroke or its progression. Subsequent FDA clearances and a recent decision to formalize regulations for such evaluations are likely to stimulate further innovation and acceptance of AI devices.
Saving time
Viz.AI Contact analyses CT images of the brain and sends a text notification by smartphone or tablet to a vascular neurologist or a neuro-interventional specialist, should a large vessel occlusion (LVO) be suspected. The algorithm automatically notifies the specialist at the same time that a review of the images is being conducted by a first-line provider. This is faster than the usual standard of care where patients wait for a radiologist to firstly review CT images and then notify a neurovascular specialist.
Retrospective study and real world data
Viz.AI, Inc., which developed the Contact application, submitted a retrospective study of 300 CT scans. This compared the performance of the image analysis algorithm and notification functionality against two trained neuro-radiologists.
Real-world evidence from a clinical study demonstrated quicker notification of a neurovascular specialist, in cases where blockage of a large vessel in the brain was suspected. In more than 95 percent of cases, the automatic notification was faster, saving an average of 52 minutes (with a range of between 6 and 206 minutes).
De Novo premarket review
The Viz.AI application was reviewed by the FDA through its De Novo premarket review process, a regulatory pathway for new types of medical devices that carry low to moderate risk, but lack a legally marketed predicate device to base a determination of equivalence. The FDA action creates a new regulatory classification, allowing other devices with the same medical imaging intended to obtain marketing authorization by 510(k) notification. One of the first areas to benefit from Viz.Ai will be AI or computer-aided triage devices, whose potential in fields such as emergency medicine is likely to be vast. Viz.AI, Inc., itself is developing Viz ICH, which uses AI to automatically detect intra-cerebral hemorrhages and triage the patient directly to the neurosurgeon on call.
Decision support for breast cancer screening
Nine months after FDA approval of Viz.AI, at the 2018 Radiological Society of North America (RSNA) annual meeting in November, Siemens Healthineers showcased the AI-based features of syngo.Breast Care, a mammography solution. syngo.Breast Care aims to provide interactive decision support for breast cancer screening.
Transpira, Siemens’ mammography reading software, is based on deep learning techniques, with training provided via over 1 million images. As a result, syngo.Breast Care’s AI-based algorithms evaluate and interpret individual lesions as well as 2-D mammograms and 3-D tomosynthesis. The system also sorts and scores cases on a 10-point scale, based on radiologist preferences of risk factors such as lesions, micro-calcifications and other abnormalities.
Siemens Healthineers aims to integrate interactive decision support into syngo.Breast Care, and reduce radiologists’ workload for the interpretation of mammograms. This has become especially challenging, given rapid growth in the use of techniques such as 3-D breast tomosynthesis.
Small firms also in play
Smaller firms have also targeted this area. ICAD’s ProFound AI, for example, also leverages AI to detect cancer in breast tomosynthesis. The software, which was FDA cleared less than a month after syngo.Breast Care was unveiled, examines every image in a tomosynthesis scan, detects malignant soft tissue densities and calcifications.
Profound AI estimates a ‘Certainty of Finding’ for each detection and, like the classification system in syngo.Breast Care, assigns Case Scores to each case to represent confidence that a detection or case is malignant. The scores are represented on a scale from 0 to 100 percent, with higher scores indicate high confidence levels in malignancy. This, in turn, is expected to improve detection, lead to fewer patient recalls and save mammographers time in reading images. This makes it geared toward screening, although it can evidently be used for diagnostic studies.
AI at inflection point
The above examples demonstrate that the use of AI is now close to an inflection point in terms of clinical decision support tools. These will provide physicians usable interactive and dynamic pathways which move beyond decision support to true evidence-based decision making, along with personalized care recommendations.
To many experts, AI seems to have been the missing link for tools that assist radiologists in improving appropriateness of follow-up recommendations for incidental findings, and thereby to enhance adherence to guidelines available at point of care. One of the consequences of such AI-assisted tools will be to reduce the variability in follow-up recommendations, as well as unnecessary imaging studies.
Diagnosis and decision support versus analysis and detection
Maximum attention to AI in imaging is currently on diagnosis and decision support. AI in areas such as quantitative analysis and assisted detection can be considered a spin-off from automation, which has been around for a longer period of time, but reinforced more recently by machine learning.
Automated quantification tools are now sufficiently mature and routinely accepted in the market. AI algorithms are used to make measurements from imaging exams and perform calculations which were previously manual and time-consuming. AI-driven quantitative analysis tools also are being used in data analytics for data mining electronic medical records, billing systems, patient scheduling and even in stand-alone scanners. Mined data range from radiation dose used by particular technologists for specific protocols to predictive analytics that pinpoint spikes in demand by day and time, and schedule back-up staff in the radiology department.
By contrast, the application of AI (and even automation) in medical fields such as computer-aided diagnosis and clinical decision support is very recent, and is likely to be some time before they become commonplace. The principal focus on AI use for image diagnosis is where timing is crucial – such as a heart attack or stroke (e.g. Viz.AI Contact). Closely related areas include tools to reduce review time for complex exams, and help triage patients needing more immediate care or other kinds of back-up.
Other new AI imaging applications
One exciting new entrant into AI in imaging is IcoMetrix, from Belgium’s IcoBrain. This FDA-cleared algorithm analyses CT scans to characterize traumatic brain injury, using deep learning to quantify the severity of such typically qualitative indicators of brain injury as hyperdense volumes, compression of the basal cisterns and midline brain shift.
Another FDA-cleared device is Cardio AIMR, which analyses MR images for cardiovascular blood flow. Its developer, Arterys, also has other AI tools to measure and track liver lesions and lung nodules, accelerate display of medical images, and interface with the common desktop Google Chrome browser to display mammograms.
The challenge of integration
Although the FDA is clearing the way for follow-on AI products, there are concerns that the process is constrained to highly specific medical imaging diagnostic reviews. Some radiologists are questioning the viability of new AI software systems, if they require scores of different contracts and integration into a hospital or enterprise imaging system – which would be a problem not only for hospital IT departments but also for legal review.
One of the ways forward is by reconfiguring approaches to enterprise imaging by streamlining workflow. Some vendors are developing bridges between different AI applications. One of the immediate goals is to have AI imaging dovetail into picture archive and communication systems (PACS) as well as vendor neutral archives. For example, Viz.ai software is designed to receive DICOM images directly from any CT scanner to a local virtual machine (VM) behind a network’s firewall.
Major firms nurture start-ups
Leading healthcare technology vendors are also starting to actively partner with smaller companies to provide a combination of in-house and third-party apps via a web-based AI app store platform. One good example of this is Siemens’ Digital Ecosystem, which offers an online menu of apps from Siemens and its partner, including some offering AI-enabled technology. Similar AI app store initiatives are also being taken by other vendors.
At RSNA 2018, where Siemens showcased syngo.Breast Care, IBM Watson said it would begin to partner with AI vendors to offer products on its new AI Marketplace, by offering standardized application programming interfaces (API) for building or integrating third party software and making it available through the IBM Cloud. Smaller vendors have seized such opportunities. French imaging agent vendor Guerbet, for instance, is working with IBM Watson Health to develop AI software to support liver cancer diagnosis and care.
IBM had initially planned to develop and launch its own AI solutions across the healthcare spectrum. However, it had to cope not only with delays in commercializing its own AI products, but small and nimbler start-ups, such as viz.AI getting ahead in obtaining FDA clearance. The biggest setback was MD Anderson ending its partnership on cancer imaging with IBM.
Other major players are also treading similar paths. GE Healthcare’s Edison platform is designed to help accelerate the development and adoption of AI and other new technologies, with clinical partners using Edison to develop and test algorithms and mate them to Edison applications and smart devices. On its part, at RSNA 2018, Philips Healthcare also launched its IntelliSpace Discovery 3.0 visualization and analysis platform to prepare patient data to train and validate deep learning algorithms. The platform is designed specifically to support imaging research.
FDA to formalize De Novo rules
Developments in AI-enabled clinical decision support, like broader AI healthcare applications, are likely to pick up after the FDA decided to formally establish regulations for the De Novo classification process in December 2018. Although the De Novo process is part of the Food and Drug Administration Modernization Act, the FDA Safety Innovation Act and the 21st Century Cures Act, it is currently not covered by any specific regulations. If finalized, the proposed rules are intended to provide clarity and transparency on the De Novo classification process.


Over recent decades, the field of telemedicine has been witness to periods of great promise, relative stasis as well as overstretch and false starts.
However, there is one telemedicine application which has seen steady, consistent growth. This is emergency telemedicine, where application development, especially teleconsultation and teleradiology, has synchronized with increasing demand for A&E as well as the forward march of telecoms technology.
From the outset, the benefits of telemedicine were self-evident in emergency care in settings such as ski resorts, highway or rail accidents, and after natural disasters. Telemedicine enabled trauma specialists to interact with overtaxed field personnel on site, to gauge the severity of injuries and provide clinical assessments on treatment or evacuation. This aspect of telemedicine was spun out off one of its first movers, the military.
Telemedicine and travel
The roots of ‘serious’ telemedicine practice can be considered to date to the 1990s. Nevertheless, medical practitioners were aware of the enormous possibilities it afforded well before this.
In the 1930s, luxury liners used marine radio-telephones to communicate with physicians about urgent cases on board. Travellers were again the core target market for the first teleradiology consultations, conducted in the 1960s by Dr. Kenneth Bird, who used a two-way/interactive television system that connected Massachusetts General Hospital to Boston’s Logan Airport to provide emergency medical care.
1994: A&E referrals fall at Belfast hospital
Among the earliest case studies on modern emergency telemedicine is a 12-month review of a 1994 link between the Royal Victoria Hospital in Belfast and a minor treatment centre (MTC) in South Westminster, London. Over the study period, the telemedicine link was actively used in only about 0.5% of cases. However, the number of patients referred to a GP fell dramatically as did those referred to A&E. Another interesting observation was an increase in confidence of the nursing staff at the Westminster MTC.
Wembley study compares outcomes, radiologists vs. teleradiologists
At the beginning of 1996, Wembley Community Hospital in London established a minor accident treatment service (MATS), supported by an advanced telemedical link to Central Middlesex Hospital. The system was run by emergency nurse practitioners based on a set of clinical protocols which consisted of prompts advising the use of telemedicine.
Two years later, a paper evaluated six months activity at the MATS, covering all patients seen – a total of 2,843, with 150 teleconsultations. After an interval of three months, 99 per cent of telemedical and 95 percent of non-telemedical cases were followed up. Interestingly, while no further problems had arisen with the telemedical group, 26 of the non-telemedicine group had consulted their GP for the same problem. Another interesting finding was that A&E teleconsultants interpreting radiographs performed better than the consultant radiologist who subsequently interpreted the original films.
Head CT scans
Similar efforts were also made in the US and continental Europe. Other than minor injuries support, another application area with near-universal acceptance in A&E practice consisted of the transmission of head CT scans to a tertiary neurosurgical centre, in order to obtain an immediate expert opinion.
Economic impact of emergency telemedicine
By the late 1990s, rather than convenience alone, the first arguments about the economic impact of emergency telemedicine had begun to appear. A 1997 paper from Hong Kong found a significant reduction in unnecessary transfers, alongside a decrease in adverse events occurring during transfer. Another study from Austria during the same year concluded that though teleradiology for CT scans was more expensive than transferring the physical scans by taxi, it was considerably quicker, and much less expensive than transferring the patient.
Growing ER costs drive US interest in telemedicine
The acceleration of growth in mobile telecoms quality onwards from the late 2000s, along with sharp falls in cost, has intensified the case for emergency telemedicine. Alongside, increased demographic pressure on emergency rooms due to an ageing population and ER staff shortfalls have strengthened this further.
ER figures have been used to make the case for emergency telemedicine in the US. 130 million people visit ERs each year, up 36 percent from 97 million in 1995. In spite of this, the number of ERs in the US dropped by 11 percent over the period.
One leading healthcare provider, Cardinal Health, estimates that the average costs of a telehealth visit at USD 40-50, compared to USD 922 for an emergency room visit and that telemedicine could eliminate nearly 1 in 5 ER visits, which corresponds in numbers to almost two-thirds of those discovered to be non-urgent. Cardinal Health also states that 20% of ER visits require follow-up care for similar conditions, while only 6% of telehealth visits do. This echoes the spirit of the findings of the Wembley Community Hospital MATS study in 1996, mentioned previously.
Waiting times and demographic pressures
The problems with emergency medical care are similar in Britain. A&E waiting times have increased substantially over recent years, with many National Health Service (NHS) units failing to meet a four-hour standard for admission and discharge at national level. The number of people going to A&E has also risen substantially. In 2016/17 there were 23.4 million attendances at A&E departments – the equivalent of 63,000 attendances each day on average, and since 2011/12, this has been growing by 1.7 per cent each year – or the equivalent of an extra 5,100 each day.
These pressures have been exacerbated by closures. One in six A&E departments are being closed or downgraded, which corresponds to 33 casualty departments in hospitals in 23 areas of the UK.
The scourge of unnecessary visits
Unnecessary visits to A&E account for 16% of the total in England, but go over 50% in areas such as Durham and Darlington. From time to time, the media has a field day, citing lists from health officials about people going to A&E with broken false nails, splinters in their fingers, emergency contraception, as well as shaving and paper cuts.
The situation is similar in the US, where over 30% of visitors discover their case is not urgent – after being attended to. Some studies have estimated that 14 to 27 percent of ER visits could be treated at facilities like retail clinics or urgent care centres, with potential savings of USD 4.4 billion.
Telehealth to ‘redesign’ emergency medicine ?
A 2017 study from the University of Warwick calls for using telehealth to “redesign” emergency medical services. It chooses best of breed cases from different continents to make three cases:
• Specialists in underserved communities
• Pre-ambulance triage
• Ambulance-based triage
Providing patient access to remote specialists in underserved communities
In its early stages, emergency telemedicine applications were motivated by the need to provide more timely diagnosis and care to patients in underserved communities, in other words those lacking hospitals with full-time emergency medicine teams.
The Warwick study cites the Western Australia Emergency Telehealth Service (ETS, which comprises over 70 regional and remote hospital EDs as a “prominent example of this type of telehealth initiative.” The WA ETS makes specialist emergency medicine physicians available via videoconferencing to support regional hospital-based clinicians with the diagnosis and treatment of acute emergency patients. Another example in the Warwick study is the Cumbria and Lancashire Telestroke Network in Britain. This remote teleconsultation service connects 15 stroke consultants to provide ‘out-of-hours’ advice from their homes to hospital sites.
More recently, conclusive evidence about some of the above advantages has been obtained from another study at the University of Iowa’s Carver School of Medicine. The study found that telemedicine-equipped rural emergency departments provided patients with access to a clinician six minutes sooner than those in hospitals without the technology, regardless of whether or not telemedicine was used to intermediate the interactions. However, when telemedicine was used, as happened in 42% of the interactions, the door-to-provider time was shortened by nearly 15 minutes. This, according to lead author Nicholas Mohr, MD, an emergency physician and associate professor at the University, could change outcomes for patients with conditions like “severe trauma, stroke, myocardial infarction.”
Pre-ambulance triage, via teleconsultation with probable primary care patients
The second application highlighted by the Warwick researchers consists of pre-ambulance triage, via a system called ETHAN (Emergency Telehealth and Navigation). This was developed by the Houston (Texas) Fire Department in 2014, and combines teleconsultation, social services and alternative transportation. Its aim is to reduce the numbers of primary-care related patients being transported directly to the ED via fire-engine (although it could apply equally to ambulance). Apart from reducing ED patient loading, ETHAN makes substantial cost savings by eliminating unnecessary fire engine/ambulance journeys – estimated at USD 2500 per trip.
ETHAN equips EMS units with a Tablet to respond to patient initiated calls. Patients are connected via secure videoconferencing software to a hospital-based emergency physician who makes a diagnosis based on vital signs measured on scene by the field crew. After outlining treatment options, the physician then makes a final decision on whether the patient should be brought to the ED by fire engine/ambulance or via taxi, or taken by the latter to a primary care facility, or instructed on home care.
There is, however, little homogeneity in pre-ambulance triage, either in the US or elsewhere. In 2013, a systematic review of 120 publications by The Norwegian Knowledge Centre for the Health Services found that there was “a lack of scientific evidence about the effects of validated pre-hospital triage systems,” and called for further research.
Ambulance-based Triage
It has long been recognized that in-ambulance triage and care for an acute emergency patient during transportation to the ED, impact positively on patient outcomes, especially with time-critical conditions such as myocardial infarction and stroke. In several respects, Europe can be considered to be ahead of the US in this application. In Tucson (Arizona), a citywide ambulance telemedicine network, was shut down in 2011 due to budgetary problems and problems of reliability with the WiFi network.
On its part, the Warwick study reports on an ambulance-based telemedicine triage system with real-time bidirectional audio-video communication, carried out in Brussels. In 90 per cent of cases, preliminary pre-hospital diagnosis was formulated and was in agreement with in-hospital diagnoses. Failures, as had been the case in Arizona, resulted mainly from limited mobile connectivity.
Standard methods of decontamination, such as Disinfector Washers (e.g. using hot alkaline solutions and surfactants), are known to be inconsistently effective in removing protein from surgical instruments. Advanced Ultrasonics offers an exciting and tantalizing alternative. Preliminary results suggest that intense cleaning using “advanced ultrasonic technology” can potentially result in disinfection without the need for any thermal or chemical methods.
by David Jones
In the UK, concerns about Creutzfeldt-Jacob Disease (CJD) date back to the mid-1980s when an outbreak of Bovine Spongiform Encephalopathy (BSE, a similar transmissible neuro-degenerative brain disease) in cattle raised concerns that the disease might be transmissible to humans. Confirmation came in 1996 [1] that BSE can indeed lead to a form of human CJD (variant (v)CJD) that particularly affected younger adults. This resulted in widespread public health concern, heightened again a few years ago when a study in the British Medical Journal [2] suggested that as many as 1 in 2000 Britons may be infected with the abnormal prion protein that causes vCJD. To date there have been 178 deaths due to vCJD in the UK with a few more elsewhere [3]. In both model experiments and in actual human studies it has been shown that the prion protein is readily transmitted on stainless steel instruments from one animal to another.
vCJD highlighted to clinicians and decontamination / sterile services professionals alike, the critical requirement to remove protein, as well as other infectious agents, from neuro-surgical and other reusable surgical instruments. In addition to the risk of patient-to-patient transferal of vCJD prions, there is a danger that bacteria hidden in or under any residual protein e.g. biofilms could also be passed on. A recent study in the journal Acta Neuropathologica [4] also highlighted the potential dangers associated with cross-contamination of neurosurgical instruments with the peptide amyloid beta (Aβ), a substance implicated in brain hemorrhages and Alzheimer’s disease.
Standard methods such as Disinfector Washers (e.g. hot alkaline solutions and surfactants) are known to be inconsistently effective in removing protein from surgical instruments [5,6] and other difficulties in ensuring consistent cleanliness has led to a move towards single use instruments. However, questions remain as to how manufacturers of single use instruments can achieve consistent cleanliness and sterility when modern, well equipped Sterile Service and Decontamination (SSD) units apparently cannot. Unfortunately, single use instruments are not always clean and sterile as recent unpublished investigations have shown.
In the UK, concerns about contamination mean that GPs and dentists, who have historically performed minor interventions such as lancing of boils, removal of small cysts and abscesses etc., are now being discouraged from doing so. This, in turn, is funnelling more patients to A&E departments, which are already under tremendous strain. Post-operative infections also add to strain on the health service, leading to extended hospital stays and bed-blocking.
There is a clear need for a new approach to improve the cleaning of surgical devices. “Commercial grade” ultrasonic cleaning systems have been available for a number of years and have been used as a first stage in the cleaning process.
Ultrasonics works via the process of cavitation. Transducers bonded to the base or side of a tank are excited by high frequency electricity causing them to expand and contract at very high speed. This mechanical action causes high speed downward flexure of the radiating tank face. The speed of this movement is too fast for the water in the tank to follow, resulting in the production of vacuum chambers. On the upward flexure the vacuums are released in the form of vacuum bubbles which rise up through the fluid until they hit an object, upon which the bubbles implode under high pressure, thus drawing away any contamination that may be on the surface of the object.
However, it has been shown that machines used in sterile services departments in the past have an erratic distribution of sound that does not consistently render instruments clear of residual protein. It was felt by many that a new way of applying ultrasound into a fluid was required. To achieve the safe cleaning of these items, the sound needs to be applied in a way that is both even as well as intense, with no gaps in activity where cleaning would not be effective.
In order to develop a new cleaning technology, a reliable method for measuring residual protein was needed and agreement reached on acceptable levels. The UK HTM 01-01 Guidance on the Management and Decontamination of Surgical Instruments [7], released in 2016, specifies that “there should be <5µg of protein in situ, on a side of any instrument tested”. In situ testing is specified since: “detection of proteins on the surface of an instrument gives a more appropriate indication of cleaning efficacy related to prion risk” than the swabbing techniques used in the past [8,9,10]. Currently the ProReveal system, from Synoptics Health, Cambridge UK, is the only in situ system on the market worldwide. As well as high levels of accuracy, the system also identifies the precise location of any remaining proteins on the instrument. To comply with UK HTM 01-01 guidance, therefore, any new cleaning system, ultrasonic or otherwise, needs to be validated against the levels of detection offered by ProReveal.
A second issue to be addressed by any ultrasonic cleaning technology is how to measure the ultrasonic activity. HTM 01-01 states that machines should be periodically tested for ultrasonic activity.
Historically, the only method available to Sterile Services Managers and AED’s for validating the activity in an ultrasonic tank has been to insert a piece of aluminium foil into the fluid for a set time and then visually analyse the indentations in the foil to determine the ultrasonic activity. This is a somewhat inaccurate way of validating what is a critical phase in the decontamination process. Troughs of sound can be either macroscopic or microscopic and, as such, the reliance on sight alone is unacceptable when such high levels of consistent cleanliness are expected.
With both these issues in mind, Alphasonics (a Liverpool/UK company with over 25 years’ experience in the field of ultrasonic cleaning systems) launched the ‘Medstar’ project with a view to developing ‘advanced ultrasonic technology’ for cleaning surgical equipment. The project started in 2013 but it was not until 2015 when a ProReveal was purchased that substantive advances were made. Progress then accelerated quickly and over a 3-year period, a point was reached whereby instruments could be rendered “completely” free of residual protein, as assessed by ProReveal technology.
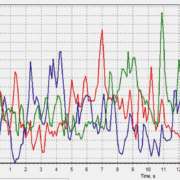
To overcome the problems around accurately measuring ultrasonic activity, the world’s first Cavitation Validation Device (CVD) was developed from 2016 to 2018 which, for the first time, allows the validation of ultrasonic cleaning devices by listening exclusively for cavitation noise.
CVDs are included within most Medstar systems and the below graphs show how Medstar devices perform compared to existing ‘commercial grade’ ultrasonic cleaners (Data on File).
It is this unique, intense ultrasound technology that is so effective in removing protein residue from medical devices, as measured by the in situ ProReveal method. To assess the effect on removal of bacteria, a UKAS (UK Accreditation Service) accredited laboratory was engaged to carry out independent trials. Instruments were contaminated by the laboratory, first with Enterococcus faecium and Staphlyococcus aureus (as specified within ISO15883 annex N- “test soils and methods for demonstrating cleaning efficacy”) and then with “dirty” conditions (specified in ISO13727). They were then cleaned in a Medstar device. Since all residual protein was being removed, the question arose: was the (now exposed) bacteria also being removed by the intense ultrasound?
Work is on-going, but preliminary results suggest that intense cleaning using ‘advanced ultrasonic technology’ can potentially result in disinfection without the need for any thermal or chemical methods.
Medstar devices have several other features to allow compliance with UK HTM01-01 guidance, such as the Generator Output Monitoring System- which constantly monitors the generator output and adjusts the input accordingly, thus ensuring that the system is always performing optimally. The CVD device is then used for periodic independent validation.
Advanced Ultrasonics offers an exciting and tantalizing alternative to thermal disinfection devices. The HTM01-01 UK guidelines are only the start of things to come and it is already widely recognized that the 5µg limit set out in the guideline is still too high. The many trials undertaken by the manufacturer have clearly shown that the Medstar range of equipment leaves no more than 0.5µg of residual protein per side on an instrument and as such renders the bacteria fully exposed to the intense, very even, action of the ultrasound and enzymatic chemicals.
High throughput systems are also available that would be of great benefit to single-use instrument manufacturers and SSD units alike. These systems will deliver a consistently lower residual protein count and a better log reduction than thermal disinfection devices.
References
1. John Collinge, Katie CL Sidle, Julie Meads, James Ironside, Andrew F Hill. Molecular analysis of prion strain variation and the aetiology of “new variant” CJD. Nature, 1996; 383(6602), 685. doi:10.1038/383685a0
2. Gill O, Spencer Y, Richard-Loendt A, Kelly C, Dabaghian R, Boyes L, Linehan J, et al. Prevalent abnormal prion protein in human appendixes after bovine spongiform encephalopathy epizootic: large scale survey. British Medical Journal, 2013; 347, 11.
3. See www.cjd.ed.ac.uk/sites/default/files/figs.pdf
4. Jaunmuktane Z, Quaegebeur A, Taipa R, Viana-Baptista M, Barbosa R, Koriath C, Sciot R, et al. Evidence of amyloid-β cerebral amyloid angiopathy transmission through neurosurgery. Acta Neuropathologica, 2018; 135(5), 671–679. doi:10.1007/s00401-018-1822-2
5. Murdoch H, Taylor D, Dickinson J, Walker JT, Perrett D, Raven NDH, Sutton JM.
Surface de-contamination of surgical instruments – an ongoing dilemma. Journal of Hospital Infection 2016; 63: 432-438
6. Baxter RL, Baxter HC, Campbell GA, Grant K, Jones A, Richardson P, Whittaker G. Quantitative analysis of residual protein contamination on reprocessed surgical instruments. J Hosp Infect 2006; 63, 439-444.
7. Department of Health and Social Care. Health Technical Memorandum (HTM) 2006; 01-01: management and decontamination of surgical instruments (medical devices) used in acute care.. Available: https://www.gov.uk/government/publications/management-and-decontamination-of-surgical-instruments-used-in-acute-care. Last accessed July 2018.
8. Nayuni N, Cloutman-Green E, Hollis M, Hartley J, Martin S, Perrett D. A critical evaluation of ninhydrin as a protein detection method for monitoring surgical instrument decontamination in hospitals. J Hospital Infection 2013; 84 97-102
9. Nayuni N, Perrett D. A comparative study of methods for detecting residual protein on surgical instruments. Medical Device Decontamination (incorporating the IDSc Journal) 2013; 18 16-20
10. Perrett D, Nayuni N. Efficacy of current and novel cleaning technologies (ProReveal) for assessing protein contamination on surgical instruments 2014; Chapter 22 in Decontamination in Hospitals and Healthcare Edited by Dr. J.T. Walker, Woodhead Publishers, Cambridge, UK.
The author
David Jones
Alphasonics, Liverpool, UK
www.alphasonics.co.uk
Prins Hendrikstraat 1
5611HH Eindhoven
The Netherlands
info@interhospi.com
PanGlobal Media IS not responsible for any error or omission that might occur in the electronic display of product or company data.
