

Telemedicine has been around for many years, evolving in tandem with technological change and improvements. In essence, telemedicine delivers healthcare services by means of technology, in cases where the healthcare professional cannot attend to the patient physically. Tele-anesthesia takes it a step further by doing pre-operative consultations by means of telemedicine systems. In this article, the authors report of the growing use of tele-anesthesia.
by Dr Nora Terrasini, Dr Erik Arbeid, Dr Riccardo Taddei, Dr Cedrick Zaouter, Dr Shantale Cyr and Dr Thomas M Hemmerling
What is telemedicine?
Telemedicine is defined as the delivery of healthcare and sharing of medical knowledge over a distance, using telecommunications systems [1]. The World Health Organization gives a more extensive definition of what should be considered as telemedicine and describes it as
Partial support for patients with respiratory failure can be provided with invasive mechanical ventilation or non-invasive mechanical ventilation. The role of non-invasive positive pressure ventilation (NPPV) in preventing intubation for various conditions has been well studied. Less well studied is the role for NPPV in the weaning and peri-extubation period.
by Dr Brooks A. Fallis and Dr Karen E. A. Burns
Mechanical ventilation is essential for supporting patients through episodes of respiratory failure by unloading respiratory muscles and improving gas exchange. While potentially lifesaving, invasive mechanical ventilation with an endotracheal tube or tracheostomy can be associated with important harm, in part due to complications such as ventilator associated pneumonia (VAP). VAP has been shown to increase morbidity and trends towards increasing mortality [1].
Critical care physicians strive to extubate patients as early as possible, while minimising the risk of re-intubation, which has been shown to be independently associated with increased risk of developing VAP [2]. Spontaneous breathing trials (SBT) are used to decide if a patient has been weaned. An SBT involves a focused assessment of a patient

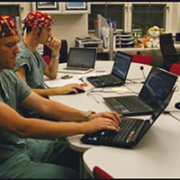
The very first intensive care units (ICUs), introduced towards the end of the 19th century, consisted of a few beds reserved for the sickest patients and put together in one area of the general hospital ward so that the patients could be watched more closely. Patients continued to be treated by their admitting physician with consultation by other specialists as dictated by the course of their disease. Later, separate rooms were created to gather together the special monitoring and organ support equipment and specially trained nursing and medical staff considered necessary for the optimal management of critically ill patients.
Over the years, especially in larger hospitals and more commonly in the United States than in other countries, subspecialty ICUs have developed, catering for specific groups of patients, such as those with neurological, respiratory, cardiac, surgical, trauma diagnoses. This division of intensive care into subspecialties reflects a general trend across medicine towards the creation of increasingly specialized subspecialties. In the United States, one third of all ICUs are now (sub)specialty units. But is there any evidence that such units provide better care than general, multidisciplinary ICUs catering for all critically ill patients regardless of diagnosis?
by Prof. Jean-Louis Vincent
Benefits of subspecialty ICUs
Proponents of specialized ICUs suggest that patient outcomes can be improved in such units because they are managed by staff with increased expertise and training in the particular field of diagnosis. Such units are thus able to provide more focused, relevant care. However, although highly trained in their particular specialty, staff in such units may be less experienced in diagnosing and managing other systemic complications of critical illness. There is relatively little data available comparing the benefits of specialty versus general ICUs. In one study, patients with intracerebral hemorrhage had improved survival rates when admitted to a specialized neurosurgical ICU compared to a general ICU [1]. However, in another analysis, admission to a diagnosis-appropriate specialty ICU was associated with no survival benefit compared to admission to a general ICU for a selection of common diagnoses, including acute coronary syndrome, ischemic stroke, intracranial hemorrhage, abdominal surgery, and coronary-artery bypass graft surgery [2]. Interestingly, admission to a diagnosis-inappropriate specialty ICU, e.g., a renal patient admitted to a neurosurgical ICU because the renal ICU was full, was associated with increased mortality rates [2]. Performing such comparative studies is, however, fraught with difficulty, largely because there is no set definition of a

The world of healthcare is changing. The prevalence of chronic diseases is increasing as our population is ageing, but there will be fewer taxpayers to maintain the current healthcare systems. We have increasing demand for expensive technologies, yet the number of healthcare professionals is decreasing. As an important step towards fostering the widespread adoption of eHealth throughout the EU, the European Commission adopted on December 6th, 2012 the eHealth Action Plan 2012-2020
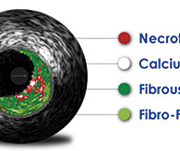
Intravascular Ultrasound (IVUS) provides images of the insides of blood vessels for the diagnosis and treatment of cardiovascular disease. Although the roots of IVUS date back a quarter century, it is only recently that physicians have begun to take serious cognizance of its potential.
Improving PCI outcomes
The growth in interest in IVUS is being driven by changes in the way for treating acute coronary syndrome (ACS). ACS is a common complication of coronary heart disease, which is the leading cause of death in industrialized countries.
The typical approach to treat ACS consists of percutaneous coronary intervention (PCI): catheter angiography, balloon angioplasty and the use of stents. However, the proponents of IVUS have been making a strong case about its utility to improve PCI outcomes, including those offered by the latest generation of drug-eluting stents (DES).
IVUS consists of a miniaturized ultrasound imaging device. This is mounted on a catheter which is threaded across an artery to provide both cross-sectional and longitudinal views. It thus reveals not only the shape and amount of plaque but the deployment and expansion of a stent, too. Such information is not accessible via standard angiography. The main area for application is coronary arteries. Growing (if still far smaller) areas consist of peripheral arteries as well as intra-cardiac imaging.
State-of-the-art IVUS systems use spectral backscatter and frequency analysis to classify plaque (distribution, burden and calcification) and are claimed to achieve up to 97% accuracy. They are also used to plan for treatment with stents
Prins Hendrikstraat 1
5611HH Eindhoven
The Netherlands
info@interhospi.com
PanGlobal Media IS not responsible for any error or omission that might occur in the electronic display of product or company data.
