Carestream Health is providing healthcare facilities with a new floor-mount option for the DRX-Compass X-ray System. This option delivers an innovative, flexible and efficient medical imaging solution to sites that are unable to accommodate an overhead tube crane.
It is ideal for community, rural and private hospitals. It is also well suited for urgent care centers, orthopaedic and large radiology practices.
A good option for smaller budgets
“The free-standing tube mount eliminates the need for ceiling rails, but still provides the wall stand, table and console features, the same as the overhead tube crane,” said Jing Chu, Worldwide Product Marketing Manager at Carestream.
“This option will offer smaller facilities or sites with tighter budgets the ability to use the DRX-Compass and put Carestream’s exceptional image capture and processing to work.”
Advanced features
The Carestream DRX-Compass X-ray System (see video of DRX-Compass system) is an upgrade-friendly unit with a broad array of advanced features and options to meet changing needs. It has vertical auto-tracking and auto-centring, as well as an optional tilting wall stand to support a wide range of exams. Developed for easy positioning, this system was designed to decrease set-up time and increase throughput for every facility. Its intuitive, graphical user interface reduces training time for radiographers and allows for a secure, swipe-and-go login. The auto long-length imaging option is especially useful for patients who have trouble standing or young children who are unable to hold still for long periods of time.
“Whatever your modality right now, and wherever you need to go in the future, we have the upgrade strategy to get you there – seamlessly,” Chu said. “The DRX-Compass is designed to keep costs in line with a facility’s needs by being scalable and upgradable.”
Bridge to move from analogue to digital
With the ability to select components for specific locations, the system can easily adapt to space requirements. The DRX-Compass offers a bridge for healthcare facilities looking to move from an analogue or retrofitted X-ray room to a digital system. Through Carestream’s ImageView clinical acquisition software, powered by Eclipse image processing, healthcare facilities can add capabilities to their DRX-Compass systems as needed over time.
https://interhospi.com/wp-content/uploads/sites/3/2021/05/Carestream-DRX-Compass-X-ray_web.jpg9561701panglobalhttps://interhospi.com/wp-content/uploads/sites/3/2020/06/Component-6-–-1.pngpanglobal2021-05-25 08:01:252021-05-25 08:01:25Carestream offers new floor-mount option for DRX-Compass X-ray system
Jeff Tabor, associate professor of bioengineering in Rice’s Brown School of Engineering (Credit: Jeff Fitlow/Rice University)
In an important step toward the clinical application of synthetic biology, Rice University researchers have engineered a bacterium with the necessary capabilities for diagnosing a human disease.
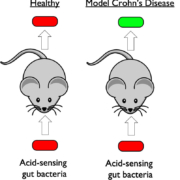
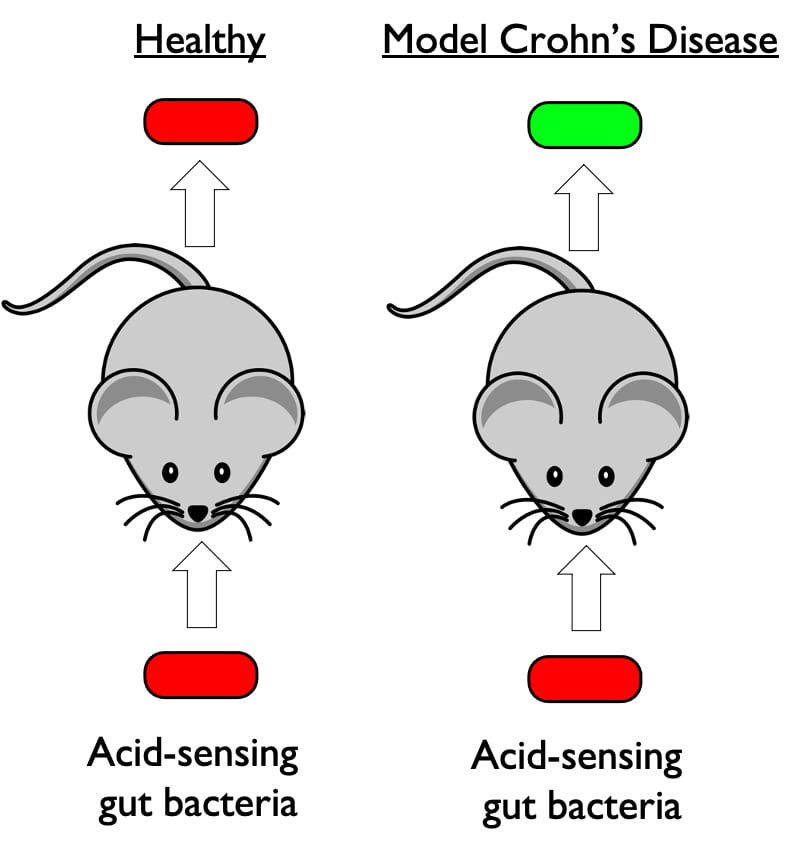
The engineered strain of the gut bacteria E. coli senses pH and glows when it encounters acidosis, an acidic condition that often occurs during flareups of inflammatory bowel diseases like colitis, ileitis and Crohn’s disease.
Rice University researchers engineered a strain of the gut bacteria E. coli to detect gastrointestinal acidosis. The organism produces fluorescent molecules that allow researchers to see it with standard optical equipment. Under normal conditions (left) it produces molecules that glow red. When it encounters acidic conditions (right), it glows green, and the brightness of the glow reflects the level of acidity. (Image courtesy of Jeff Tabor/Rice University)
Researchers at the University of Colorado (CU) School of Medicine used the Rice-created organism in a mouse model of Crohn’s disease to show acidosis activates a signature set of genes. The corresponding genetic signature in humans has previously been observed during active inflammation in Crohn’s disease patients. The results are available online in the Proceedings of the National Academy of Sciences.
Colours that show up in the toilet
Study co-author Jeffrey Tabor, whose lab engineered the pH-sensing bacterium, said it could be reprogrammed to make colours that show up in the toilet instead of the fluorescent tags used in the CU School of Medicine experiments.
“We think it could be added to food and programmed to turn toilet water blue to warn patients when a flareup is just beginning,” said Tabor, an associate professor of bioengineering in Rice’s Brown School of Engineering.
Over their 3.5 billion-year history, bacteria have evolved countless specific and sensitive genetic circuits to sense their surroundings. Tabor and colleagues developed a biohacking toolkit that allows them to mix and match the inputs and outputs of these bacterial sensors. The pH-sensing circuit was discovered by Rice Ph.D. student Kathryn Brink in a 2019 demonstration of the plug-and-play toolkit.
pH sensor
PNAS study co-authors Sean Colgan, the director of the CU School of Medicine’s mucosal inflammation program, and Ian Cartwright, a postdoctoral fellow in Colgan’s lab, read about the pH sensor and contacted Tabor to see if it could be adapted for use in a mouse model of Crohn’s disease.
“It turns out that measuring pH within the intestine through noninvasive ways is quite difficult,” said Colgan, the Levine-Kern Professor of Medicine and Immunology in the CU School of Medicine.
So Brink spent a few weeks splicing the necessary sensor circuits into an organism and sent it to Colgan’s lab.
“Normally, the pH in your intestines is around seven, which is neutral, but you get a lot of inflammation in Crohn’s disease, and pH goes to something like three, which is very acidic,” Tabor said.
Colgan and colleagues have studied the genes that are turned on and off under such conditions and “needed a tool to measure pH in the intestine to show that the things they were observing in in vitro experiments were also really happening in a live animal,” Tabor said.
Biological tool
“Colonizing this bacterial strain was the perfect biological tool to monitor acidosis during active inflammation,” Colgan said. “Correlating intestinal gene expression with the bacterial pH sensing bacteria proved to be a useful and valuable set of biomarkers for active inflammation in the intestine.”
Tabor said he believes the pH-sensing bacterium could potentially be advanced for human clinical trials in several years.
https://interhospi.com/wp-content/uploads/sites/3/2021/05/CROHNS-mouse_web.jpg856804panglobalhttps://interhospi.com/wp-content/uploads/sites/3/2020/06/Component-6-–-1.pngpanglobal2021-05-19 11:35:382021-05-19 11:35:38Researchers create bioengineered organism that could diagnose Crohn’s disease flareups
Australian study shows that savings made from shorter stays are double the cost of hiring more staff
A study across 55 hospitals in Queensland, Australia suggests that a recent state policy to introduce a minimum ratio of one nurse to four patients for day shifts has successfully improved patient care, with a 7% drop in the chance of death and readmission, and 3% reduction in length of stay for every one less patient a nurse has on their workload.
The study of more than 400,000 patients and 17,000 nurses in 27 hospitals that implemented the policy and 28 comparison hospitals is published in The Lancet. It is the first prospective evaluation of the health policy aimed at boosting nurse numbers in hospitals to ensure a minimum safe standard and suggests that savings made from shorter hospital stays and fewer readmissions were double the cost of hiring more staff.
Despite some evidence that more nurses in hospitals could benefit patient safety, similar policies have not been widely implemented across the globe, partly due to an absence of data on the long-term effects and costs, as well as limited resources. In recent years, Scotland, Wales, and Ireland have mandated numbers of patients per nurse, but strategies to improve nursing levels remains debated worldwide.
Study fills data gap
“Our findings plug a crucial data gap that has delayed a widespread roll-out of nurse staffing mandates. Opponents of these policies often raise concerns that there is no clear evaluation of policy, so we hope that our data convinces people of the need for minimum nurse-to-patient ratios by clearly demonstrating that quality nursing is vital to patient safety and care,” says lead author, Professor Matthew McHugh of the University of Pennsylvania School of Nursing, USA.
In 2016, 27 public hospitals in Queensland were required to instate a minimum of one dedicated nurse for every four patients during day shifts and one for every seven patients for night shifts on medical-surgical wards.
The research team collected data from those 27 Queensland hospitals that instated ratios and from 28 other hospitals in the state that did not, at baseline in 2016 and at follow-up in 2018 (two years after the policy was implemented). Only nurses in direct contact with adult patients in medical-surgical wards were included – data from patients in birthing suites and psychiatric units were not assessed in the study.
Researchers used patient data to assess demographics, diagnoses, and discharge details for patients, as well as length of hospital stay. These data were then linked to death records for 30 days following discharge, and to readmissions within seven days of discharge.
The researchers sent an email survey to nurses in each hospital to ask about the numbers of bedside nurses and patients on their most recent shift. The responses were used to establish the numbers of nurses per patient and then averaged across wards and hospitals. Responses were received from 8,732 nurses (of a possible 26,871) at baseline in 2016, and 8,278 (of a possible 30,658) in 2018.
The study includes baseline data for 231,902 patients (142,986 in hospitals that implemented the policy and 88,916 in comparison hospitals), and for 257,253 patients (160,167 in hospitals that implemented the policy and 97,086 in comparison hospitals) after the policy was brought in.
Comparison hospitals had no change in staffing, with six patients per nurse in 2016 and the same ratio (1:6) in the follow-up period in 2018. Intervention hospitals averaged five patients per nurse at baseline in 2016, with a reduction to four per nurse after the policy implementation.
Patient deaths
To compare the changes in outcomes in the intervention and comparison hospitals over time, the researchers estimated the odds of dying within 30 days of admission and of being readmitted within seven days of discharge, and the additional length of stay, after adjusting for factors such as patient age, sex, existing health conditions and hospital size. They found that the chance of death rose between 2016 and 2018 by 7% in hospitals that did not implement the policy, and fell by 11% in hospitals that did implement the policy.
Readmissions
The chances of being readmitted increased by 6% in the comparison hospitals over time, but stayed the same in hospitals that implemented the policy. Between 2016 and 2018, the length of stay fell by 5% in the hospitals that did not implement the policy, and by 9% in hospitals that did.
Nurse workloads
Further analyses found that when nurse workloads improved by one less patient per nurse, the chance of death and readmissions fell by 7%, and the length of hospital stay dropped by 3%.
Using their modelling to predict figures that would have been expected without the policy in place, the researchers estimated that there could have been 145 more deaths, 255 more readmissions and 29,222 additional days in hospital in the 27 hospitals that implemented the policy between 2016 and 2018.
Financial impact of employing more nurses
To calculate the financial impact of the staffing policy, the researchers used state data to estimate the cost of funding the 167 extra staff needed to reduce workload by one patient per nurse at approximately $33,000,000 (AUD) in the first two years. Based on Australian health economic data, they further estimated that preventing readmissions and reducing lengths of stay resulted in an approximate saving of $69,150,858 in the 27 hospitals across the two years following the mandate.
“Part of the reluctance to bring in a minimum nurse-patient ratio mandate from some policy-makers is the expected rise in costs from increased staffing. Our findings suggest that this is short-sighted and that the savings created by preventing readmissions and reducing length of stay were more than twice the cost of employing the additional nurses needed to meet the required staffing levels – a clear return on investment. Often, policy-makers are concerned about whether they can afford to implement such a policy. We would encourage governments to look at these figures and consider if they can afford not to,” says Professor Patsy Yates of the Queensland University of Technology School of Nursing, Australia.
Study limitations
The authors note that there are a number of limitations associated with the study. Hospitals in the research were not randomly assigned to comparison or intervention groups, as only 27 hospitals in the state were mandated to follow the policy. Furthermore, the hospitals included in both groups were not matched for size or patient demographics and health conditions, although this is accounted for in adjusted analyses.
Access the study: Effects of nurse-to-patient ratio legislation on nurse staffing and patient mortality, readmissions, and length of stay: a prospective study in a panel of hospitals. The Lancet. May 11, 2021. https://doi.org/10.1016/S0140-6736(21)00768-6
https://interhospi.com/wp-content/uploads/sites/3/2021/05/nurse7.jpg17011134panglobalhttps://interhospi.com/wp-content/uploads/sites/3/2020/06/Component-6-–-1.pngpanglobal2021-05-19 08:07:492021-05-19 08:07:49More nurses lead to shorter hospital stays, less readmissions and fewer patient deaths
By Tara Hurst
Lecturer, Biomedical Science, Birmingham City University
The development of several COVID vaccines in less than a year has given us all hope of a release from the pandemic. Now the goal has shifted to ensuring widespread vaccine coverage is achieved as quickly as possible around the globe.
However, it is unlikely that any of the vaccines will be 100% effective at stopping transmission or infection. There is a small risk that some fully vaccinated people will get infected. This is known as a “breakthrough infection” – and it’s entirely expected.
It is important to realise the limitations of vaccines. No vaccine offers full protection to everyone who receives it. The measles vaccine has been highly effective at preventing infection, leading to the virus being nearly eradicated in some countries.
Yet there are infections reported even in populations with widespread vaccination. These infections occur not only in the unvaccinated; there are cases of breakthrough infections in fully vaccinated people.
The seasonal flu vaccine offers protection from the circulating viruses. But the circulating flu viruses vary, and vaccinated people may still get ill but have less severe illness.
This is possibly because different arms of the immune response produce different defences, namely antibodies, which are Y-shaped proteins that lock onto germs and neutralise them, and T cells, which find and destroy infected cells. Antibodies are typically raised against the more variable proteins on the surface of the virus, while the more consistent proteins inside the virus are targeted by the T cells. T cells are important for limiting the severity of illness.
For SARS-CoV-2 (the virus that causes COVID-19) there is anecdotal evidence, including from Seychelles, of breakthrough infections, but little has yet been published in scientific journals. A recent report in the New England Journal of Medicine described two COVID-19 cases following vaccination, with both showing mild symptoms that resolved within one week.
And a study from Stanford University, which is yet to be reviewed by other scientists, describes 189 post-vaccination COVID cases out of 22,729 healthcare workers, but attributes at least some of these to partial vaccination. Vaccination will probably make the disease less severe should such breakthroughs occur.
Several explanations
There are several possible explanations for breakthrough infections. The human immune response is encoded in our DNA and varies from person to person. This variability helps us to respond to an array of germs. But the effectiveness of these responses is also variable. This could also be due to several things, including poor health, medication or age.
The ageing immune system does not respond to new antigens (foreign substance that causes your immune system to produce antibodies against it) and vaccines as well as younger immune systems. For one COVID vaccine, there was a measurable difference in the concentration of neutralising antibodies in the elderly compared with younger adults. Some of the elderly participants had no neutralising antibodies at all after both doses of the vaccines.
Another reason for breakthrough infections is due to viral variants that escape immune detection and flourish even in vaccinated people. A virus, especially an “RNA virus” such as SARS-CoV-2, is expected to mutate and give rise to variants, some of which may be more easily transmitted. These variants may also be more or less effectively neutralised by the immune system since the mutations could alter the parts of the virus that are recognised by antibodies and T cells.
A new SARS-CoV-2 variant identified in India (B16172) is thought to make the virus more transmissible and this is a cause for concern in light of the COVID crisis unfolding there. Despite the absence of scientific studies, there are many reports in the media of frequent breakthrough infections and the B16172 variant is blamed, but this has yet to be proved.
In the one study, done on post-vaccine infections with SARS-CoV-2 in California, there was no significantly higher risk of infection due to the variants circulating in that region. Despite the evidence that the vaccines work well against the variants, the rapid increase in the proportion of cases in the UK that are due to B16172 as compared to the dominant Kent strain (B117) has meant that it has been raised to a variant of concern by Public Health England.
While widespread vaccination remains the pandemic end game, it bears mentioning that this is unlikely to prevent all infections. Those who develop COVID after vaccination will probably have a milder illness, and so the risk of breakthrough infections should not deter us from using the current vaccines. Further study into the causes of breakthrough SARS-CoV-2 infections could help scientists to refine COVID vaccines or the schedule of booster doses.
https://interhospi.com/wp-content/uploads/sites/3/2021/05/covid_vaccine_web.jpg11341701panglobalhttps://interhospi.com/wp-content/uploads/sites/3/2020/06/Component-6-–-1.pngpanglobal2021-05-18 11:21:252021-05-18 11:21:25COVID vaccines: some fully vaccinated people will still get infected – here’s why
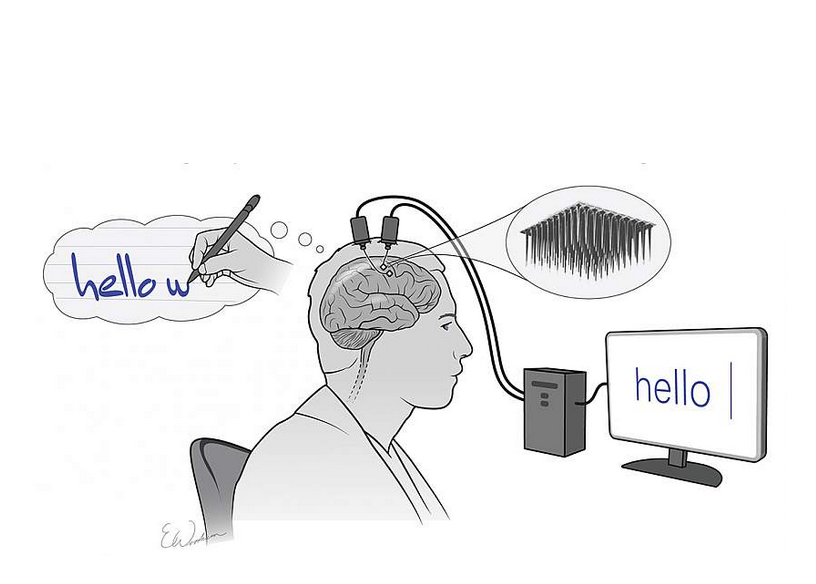
Thoughts turned into text: Two implanted electrode arrays record the brain activity produced by thinking about writing letters. This information is then collected and processed in real-time by a computer, which converts that data into words on a screen. Courtesy Shenoy lab & Erika Woodrum (artist)
Scientists have developed a brain-computer interface (BCI) which for the first time enables neural signals associated with handwriting to be decoded and turned into text in real time.
This breakthrough in BCI technology has the potential to enable paralysed or paraplegic individuals – unable to write or speak – to communicate in writing, at speed, in real time.
The study was published in Nature, May 12.
The researchers developed an intracortical BCI that decodes attempted handwriting movements from neural activity in the motor cortex and translates it to text in real time, using a recurrent neural network decoding system.
They tested the device in a participant with paralysis which in essence enabled him to type without using his hands. By thinking about handwriting letters, the researchers were able to decode the neural signals with an algorithm which turned the letters into typed text on a screen in real time.
The study participant typed 90 characters per minute – more than double the previous record for typing with such a BCI. However, previous studies had not used decoded neural handwriting signals. They had instead used thought-controlled cursor movements on a virtual keyboard.
Neural signals associated with handwriting
Study coauthor Krishna Shenoy, a Howard Hughes Medical Institute (HHMI) investigator at Stanford University and his team have in recent years been studying neural activity associated with speech in an effort to reproduce it. However, they had not considered trying to decode neural signals associated with handwriting, says Frank Willett, an HHMI research specialist and neuroscientist in Shenoy’s group.
First, the participant was asked to copy letters that were displayed on the screen, which included the 26 lower-case letters along with some punctuation: “>” which was used as a space and “~” which was used as a “full stop.” At the same time, implanted electrodes recorded the brain activity from approximately 200 individual neurons associated with handwriting that responded differently while he mentally “wrote” each individual character. After a series of training sessions, the BCI’s computer algorithms learned how to recognize neural patterns corresponding to individual letters, allowing the participant to “write” new sentences that hadn’t been printed out before, with the computer displaying the letters in real time.
“This method is a marked improvement over existing communication BCIs that rely on using the brain to move a cursor to ‘type’ words on a screen,” said Willett, the study’s lead author. “Attempting to write each letter produces a unique pattern of activity in the brain, making it easier for the computer to identify what is being written with much greater accuracy and speed.”
Level of flexibility
This system also provides a level of flexibility that is crucial to restoring communication. Some studies have gone as far as attempting direct thought-to-speech BCIs that, while promising, are currently limited by what is possible through recordings from the surface of the brain which averages responses across thousands of neurons.
“Right now, other investigators can achieve about a 50-word dictionary using machine learning methods when decoding speech,” said Dr. Shenoy. “By using handwriting to record from hundreds of individual neurons, we can write any letter and thus any word which provides a truly ‘open vocabulary’ that can be used in almost any life situation.”
Although it is still relatively early days for this technology, it offers the potential to help those who have completely lost the ability to write and speak.
In the future, Dr. Shenoy’s team intends to test the system on a patient who has lost the ability to speak, such as someone with advanced ALS. In addition, they are looking to increase the number of characters available to the participants (such as capital letters and numbers).
The participant is part of a clinical trial, called BrainGate2, which is being conducted by a collaboration of internationally recognized laboratories, universities, and hospitals working to advance brain-computer interface technologies.
Reference
Willett, F.R., Avansino, D.T., Hochberg, L.R. et al. High-performance brain-to-text communication via handwriting. Nature593, 249–254 (2021). https://doi.org/10.1038/s41586-021-03506-2
https://interhospi.com/wp-content/uploads/sites/3/2021/05/bci.png584816panglobalhttps://interhospi.com/wp-content/uploads/sites/3/2020/06/Component-6-–-1.pngpanglobal2021-05-13 12:42:292021-05-13 12:42:29Brain-to-text: Researchers develop brain-computer interface that turns neural signals into typed text in real time
A 14-year-old boy has received a living liver donation from his elder brother at Cleveland Clinic Abu Dhabi, an integral part of Mubadala Health, becoming the youngest patient to undergo the operation in the hospital’s history.
Montasir Elfatih Mohyeldin Taha was diagnosed with biliary atresia in infancy, a condition where the bile ducts outside the liver fail to form during fetal development, not allowing the bile to reach the small intestine where it helps in the digestion of fat. At 10 months, he had to undergo the Kasai procedure, which is done to connect a loop of small bowel directly to the liver so that the bile can drain into it. Montasir’s doctors back home in Sudan knew that it was only a matter of time before he would have to undergo a liver transplant, an inevitable consequence for most children who have this procedure.
Portal hypertension
Earlier this year, Montasir’s symptoms and blood tests revealed that he had started developing liver failure and was suffering from portal hypertension, an increase in the pressure within the vein that carries blood from the digestive organs to the liver, resulting in varicose veins in his esophagus. Seeing the high risk of potential complications, his doctors in Sudan recommended that he undergo a liver transplant at Cleveland Clinic Abu Dhabi.
Dr. Luis Campos, the Director of Liver Transplant and Hepatobiliary at Cleveland Clinic Abu Dhabi, who was part of the interdisciplinary team that cared for Montasir, says this was one of the most complex living donor liver transplant surgeries that they have performed at the hospital.
“There were additional nuances that had to be taken into consideration because of his age, which made it even more challenging. Factors such as height and weight impact the surgery and after-care, and determine the dose of immunosuppressive medication during and after the transplant. There is also a risk of other infectious complications in pediatric liver transplant that do not apply to adult surgeries,” says Dr. Campos.
Multidisciplinary medical team
The multidisciplinary medical team at Cleveland Clinic Abu Dhabi studied the case and evaluated Montasir’s mother and brother for a match in February. After careful discussion with colleagues in the US-based Cleveland Clinic, doctors here decided that his sibling would be a more suitable match.
“My little brother needed me. I was very relieved when I was told that I can help be the cure to his illness. This was one of the easiest decisions that I have had to make,” says Khalifa Elfatih Mohyeldin Taha. “My father passed away six months back and as the eldest son in the family, it was my responsibility to save him.”
Kasai procedure
Dr. Shiva Kumar, the Chair of Gastroenterology and Hepatology in the Digestive Disease Institute at Cleveland Clinic Abu Dhabi, who was also part of the patient’s care team, says one of the biggest challenges during Montasir’s transplant was posed by the young patient’s Kasai procedure.
“While the Kasai procedure is commonly performed to prolong the need for a liver transplant in children, this is a major operation and makes the transplant more challenging to perform,” says Dr. Kumar.
“However, the surgeries of both brothers were successful and without complications. Montasir received a left lobe graft from his brother. This is a smaller portion of the liver than if we were transplanting a right lobe graft. This makes it a safer operation for the donor and helps them recover faster.”
Immunosuppressive regimen
The brothers are on their way to a full recovery. Khalifa is back to his normal life now while the Cleveland Clinic Abu Dhabi care team is monitoring Montasir’s immunosuppressive regimen, which he will be on for the rest of his life.
Khalifa says he could not contain his joy when he was told that the surgery was a success. “The best part of my transplant journey was to see that Montasir’s body had accepted the new organ. My family and I are very grateful to the care team at Cleveland Clinic Abu Dhabi for saving my brother’s life.”
He also hopes that more people consider organ donation. “The feeling of giving a chance to someone to live a normal life is incomparable. Seeing the result of your donation will fill you with contentment.”
https://interhospi.com/wp-content/uploads/sites/3/2021/05/liver_transplant.jpg473850panglobalhttps://interhospi.com/wp-content/uploads/sites/3/2020/06/Component-6-–-1.pngpanglobal2021-05-13 11:24:132021-05-13 11:24:1314-year-old becomes youngest patient to receive living donor liver transplant at Cleveland Clinic Abu Dhabi
Yosi Health, a provider of digital patient scheduling, registration, payment, and communication cloud-based software solutions, has been selected by Henry Schein Medical Systems.
Henry Schein Medical Systems, a subsidiary of Henry Schein and developer of MicroMD, will integrate Yosi’s patient intake solution, Yosi Intake, with their practice management and electronic medical record software.
Contactless waiting room
Yosi Intake can create a contactless waiting room by enabling patients to register at home, helping to improve the patient experience and reduce administrative costs for the practice. The solution can help eliminate wait times and enhance the patient experience for small to large clinical practices.
“The COVID-19 pandemic has forced healthcare practices to dramatically rethink the way they interact with patients,” said Hari Prasad, CEO of Yosi Health. “Yosi Health allows these practices to streamline the patient intake process, which gives patients the assurance and confidence they need to keep current with their regularly scheduled office visits.”
MicroMD
Serving more than 10,000 physicians in primary care, as well as all major medical and surgical specialties, MicroMD offers practices a portfolio of integrated medical software solutions, including electronic claims management, accounts receivable management, patient registration and scheduling, and reporting. In addition, the portfolio includes an intuitive electronic medical record system with streamlined encounter capture and multiple charting methods.
“Yosi Health provides an exceptional, end-to-end patient experience that shoulders most of the administrative and document management load for client facilities,” explained Kristen Heffernan, General Manager at MicroMD. “Together with Yosi Health, we are helping providers reimagine healthcare, leveraging integrated technology that changes the way practices keep their patients and staff safe and modernizes the care delivery experience.”
https://interhospi.com/wp-content/uploads/sites/3/2021/05/yosi2.jpg1298806panglobalhttps://interhospi.com/wp-content/uploads/sites/3/2020/06/Component-6-–-1.pngpanglobal2021-05-12 09:12:512021-05-14 06:00:40Yosi Health’s patient intake solution selected by Henry Schein Medical Systems to create virtual waiting room
Hologic has made available in Europe 3D ultrasound imaging on the SuperSonic MACH 30 and 20 ultrasound systems. This innovation gives clinicians access to high-resolution B-mode and ShearWave PLUS elastography 3D volumes, providing additional insights and enhancing diagnostic certainty.
https://interhospi.com/wp-content/uploads/sites/3/2021/05/1A_HOLOGIC.jpg7381000HOLOGIC NVhttps://interhospi.com/wp-content/uploads/sites/3/2020/06/Component-6-–-1.pngHOLOGIC NV2021-05-06 13:42:222021-05-11 13:45:57Hologic introduces 3D breast ultrasound imaging on SuperSonic MACH Systems in Europe
Siemens Healthineers’ Atellica VTLi Patient-Side Immunoassay Analyser2 has obtained CE mark and is expected to be available later this spring. The Atellica VTLi analyser provides high-sensitivity cardiac troponin I (hs-cTnI) test results to clinicians in eight minutes using a patient’s fingerstick blood sample. With this industry first technology, Siemens Healthineers is helping to improve the […]
Royal Philips, has received U.S. FDA 510 (k) clearance for its Philips SmartCT application software. SmartCT is a key component of Philips Image Guided Therapy System – Azurion – providing interventionalists with CT-like 3D images (Cone Beam CT) to support diagnosis, therapy planning, treatment and follow-up for interventional radiology procedures.
https://interhospi.com/wp-content/uploads/sites/3/2021/05/4C_PHILIPS.jpg4741000Philips Healthcarehttps://interhospi.com/wp-content/uploads/sites/3/2020/06/Component-6-–-1.pngPhilips Healthcare2021-05-06 13:31:442021-05-11 13:41:39Philips SmartCT 3D image acquisition for Azurion system gets FDA clearance
We may ask you to place cookies on your device. We use cookies to let us know when you visit our websites, how you interact with us, to enrich your user experience and to customise your relationship with our website.
Click on the different sections for more information. You can also change some of your preferences. Please note that blocking some types of cookies may affect your experience on our websites and the services we can provide.
Essential Website Cookies
These cookies are strictly necessary to provide you with services available through our website and to use some of its features.
Because these cookies are strictly necessary to provide the website, refusing them will affect the functioning of our site. You can always block or delete cookies by changing your browser settings and block all cookies on this website forcibly. But this will always ask you to accept/refuse cookies when you visit our site again.
We fully respect if you want to refuse cookies, but to avoid asking you each time again to kindly allow us to store a cookie for that purpose. You are always free to unsubscribe or other cookies to get a better experience. If you refuse cookies, we will delete all cookies set in our domain.
We provide you with a list of cookies stored on your computer in our domain, so that you can check what we have stored. For security reasons, we cannot display or modify cookies from other domains. You can check these in your browser's security settings.
.
Google Analytics Cookies
These cookies collect information that is used in aggregate form to help us understand how our website is used or how effective our marketing campaigns are, or to help us customise our website and application for you to improve your experience.
If you do not want us to track your visit to our site, you can disable this in your browser here:
.
Other external services
We also use various external services such as Google Webfonts, Google Maps and external video providers. Since these providers may collect personal data such as your IP address, you can block them here. Please note that this may significantly reduce the functionality and appearance of our site. Changes will only be effective once you reload the page
Google Webfont Settings:
Google Maps Settings:
Google reCaptcha settings:
Vimeo and Youtube videos embedding:
.
Privacy Beleid
U kunt meer lezen over onze cookies en privacy-instellingen op onze Privacybeleid-pagina.