


We are all aware that there is a dearth of physicians both in primary healthcare and several hospital specialities in the West, an escalating problem that is particularly acute in the case of anesthesiologists. In some European countries this situation is at least partially the result of poor planning and under-investment in medical education, coupled with aggressive attempts to recruit medical professionals overseas, but there are other factors involved that must be addressed before we can hope to consider approaches that could alleviate the problem.
A major contributing factor is that today’s anesthesiologists are not only active in the operating theatre: their expertise is required during patient evaluation prior to surgery, and in critical care and pain management post-surgery. And not only has medical research augmented the number of surgical procedures that are now possible, but Europe’s increasing numbers of senior citizens, who are the most likely to suffer from non-communicable and chronic diseases, are the main beneficiaries of these innovative approaches. Inevitably this results in the demand for anesthesiologists exceeding the supply.
Another factor is that the generation of predominantly male anesthesiologists who focussed on their careers and were prepared to work in the evenings, at night and during weekends and holidays, severely limiting the time they could spend with their families, are retiring and being replaced by younger specialists who are legally entitled to work fewer hours per week and are also aware that social changes in recent decades, allowing both genders to enjoy satisfactory careers, require them to contribute practically (as well as financially) at home.
There is also a shortage of surgeons in Europe but this problem is not so acute as with anesthesiologists. Sadly this may well be because of the greater prestige enjoyed by practitioners of the former specialization, a situation which should surely be an anachronism. It is to be hoped that the primary goal of all medical professionals is to help their patients but until all specialisms are equally valued and respected for their essential contribution to patient care, some will continue to attract fewer recruits than others. There could even be a long-term solution to the problem if physicians themselves, including anesthesiologists, would value and respect non-medical healthcare professionals as they deserve. Surely the ever evolving technologies available in critical care settings and the relevant training offered could allow specialized anesthesia nurses to be trusted to administer anesthesia for certain procedures and patients, as well as sedation and pain relief, without requiring direct supervision from on high?

This was the theme for the 29th World AIDS Day on December 1st. Substantial progress has been made in developing and disseminating effective antiretroviral therapy (ART) for people diagnosed with HIV/AIDS. Indeed for the around 19 million people globally currently taking ART, the disease can be considered a chronic condition, albeit one that requires careful and continuous monitoring.
Huge strides have also been made in reducing transmission of infection. Concerted efforts by national programmes and development partners have promoted safe sex and condom use (though not without some controversy and pontification about the value of celibacy) with studies showing that this reduces HIV transmission by 85percent. Medical male circumcision, which reduces the risk of heterosexual men becoming infected by an estimated 60percent, is also becoming acceptable in high risk countries where performance of this operation is not the cultural norm. The efficacy of pre-exposure prophylaxis (PrEP) for subjects at a high risk of becoming infected with HIV, such as those with infected sexual partners, has been demonstrated and is advocated in many countries. Vertical transmission, formerly accounting for up to 45percent of babies acquiring the infection from their HIV positive mother, can now be prevented by prescribing ART to both mother and child during pregnancy, labour, delivery and breastfeeding. And programmes have been set up both to educate people who inject recreational drugs about the risks of HIV infection and to provide sterile injecting equipment to reduce the risk.
However an enormous obstacle blocking the goal to end the AIDS epidemic by 2030 is that according to the WHO an estimated 14 million people (around 40percent of all people with HIV) are unaware that they are infected with the virus. Not only are they not receiving ART, they are also unwittingly infecting others. Highly accurate rapid diagnostic tests or enzyme immunoassays are available, but many people are either geographically distant from such testing services or are too diffident to access them. So it is wonderful news that, according to WHO, twenty-three countries have so far approved policies for HIV self-testing, and many others are aiming to follow suit. Studies have shown that with such testing, performed in the privacy of one’s home with results available after 20 minutes, the number of people tested doubles. While there is great need to distribute kits to the most high risk areas, how many of us currently living in lower risk countries are celibate until we meet our life partner who has also been celibate prior to meeting us?

Danish, Finnish and Swedish organizations join forces to facilitate business partnering and networking at Arab Health 2018. At the event, 75 Nordic companies bring innovative life science solutions aiming to add sustainable value to the Middle East healthcare sectors and to build lasting relations between the Nordic participants and local stakeholders.
Business Finland, Business Sweden, Danish Health Tech Group and Global Pharma Consulting are coordinating four national pavilions at Arab Health 2018. To kick off the trade fair, the organizations announce an exclusive Nordic Business Partnering and Networking Reception for invited guests on Monday 29 January 2018 at 7-10 pm at the Sofitel Dubai Downtown.
“This is the only opportunity for stakeholders in the MENA region to talk to so many decision makers, officials and experts from the Nordics in one place in a relaxed setting,” explains Senior Consultant Paula Hassoon at Global Pharma Consulting, organizer of The Innovation Pavilion by Sweden.
“Joining forces with our Danish and Finnish colleagues to host a Nordic partnering and networking event brings added value to all of the participating companies,” she says.
Digital health from Finland
At the four national pavilions, the Nordic companies will showcase cutting-edge med-tech solutions and technologies to the MENA region. According to Meria Heikelä, Director at Business Finland and co-organiser of the Finnish pavilion, Finland ranks among the three strongest health technology economies in the world, with digital health being its largest high-tech export.
“Finland’s world-class research and technology competencies are the pinnacle of its health sector and one reason why Finland has one of the most efficient healthcare systems in the world. Preventive healthcare and rehabilitation solutions are among the key focus areas of Finland at Arab Health 2018,” explains Meria Heikelä.
Danish innovations in med-tech
With the annual Pavilion of Denmark at Arab Health and a recent business delegation visit to UAE and Saudi Arabia healthcare sectors, Danish Health Tech Group is committed to share the Danish med-tech strengths with stakeholders in the MENA region.
“In Denmark, we prioritize design and quality, and innovate through an inherent focus on public-private sector cooperation and by proactively involving patients and staff in the healthcare sector,” says Thomas Andersen, Head of Danish Health Tech Group.
Swedish world-class healthcare
While all the Danish companies are exhibiting with Danish Health Tech Group, Sweden offers two different pavilions.
The Innovation Pavilion by Sweden and the official Swedish pavilion each has representatives from 20 Swedish healthcare and life science companies.
“Sweden is known for its world-class’ innovations within the healthcare sector. Much of this success derives from the tradition of entrepreneurship through the close collaboration between the government, academia and industry,” says Fredrik Bodin, Trade Commissioner of Sweden to the UAE, co-organizer of the official Swedish pavilion.
The national pavilions at Arab Health 2018
More information to be obtained from:
Business Finland (Finpro) at www.finpro.fiBusiness Sweden’s at www.business-sweden.seDanish Health Tech Group at www.dk-healthtech.comGlobal Pharma Consulting at www.globalpharma.se
The Health Industry Summit (tHIS) 2017 hosted by China and organized by Reed Sinopharm, was held in Shanghai at the National Exhibition and Convention Center from May 15th to 18th with well over 200,000 healthcare industry professionals from more than 150 countries and regions in attendance.
Now in its third edition, tHIS has been firmly established as the world’s largest health industry event with over 350,000 square meters of exhibition space and 160 individual events and conferences. It comes at a crucial time as China drives forward its “Healthy China 2030 Plan” initiative to realize among other goals an industry growth target of RMB 16 trillion (USD 2.3 trillion, Euro 1.9 trillion) by 2030 and an increase of average citizen lifespan by 3 years to 79 years.
Key events at tHIS 2017 included China’s three top medical equipment and pharmaceutical exhibitions (CMEF, PHARMCHINA and API China) and the leading healthcare investment forum – Healthcare China 2017. This year’s investment forum was co-organized by Reed Sinopharm, JP Morgan Asset management, CICC and Sinopharm Capital and was attended by more than 1000 CEOs, investors and institutions.
The exhibition featured the entire industry value chain and showcased tens of thousands of the latest technologies and products. Emerging technologies such as VR, AR, wearables and AI featured strongly on the show floor as well as in the key forums. During tHIS 2017, the World Medical Robots Innovation and Development Summit was held to reflect the growing trend for robotics and AI applications.
Over 7000 exhibiting companies from 30 countries were at the show including medical device giants like GE, United Imaging, Siemens, Philips and Mindray as well as major pharmaceutical groups in China including Sinopharm, Shanghai Pharma and CR Pharmaceuticals. The majority of the most innovative companies in the medical field choose CMEF as their global or Asia Pacific new product launch platform and more than 600 new product launches took place during the 4 days of the show. Among the new products released, United imaging launched its uVR 4D vision explorer platform, enabling more detailed dissect structure and spatial information, while GE launched its first cloud-based digital application for medical equipment management APM (asset performance management), which was developed by their China team. BGI also attended with their gene sequencer BGISEQ-500, a benchtop high-throughput open sequencing platform that provides end-to-end solutions.
Natural Health and Nutrition Expo were among the fastest growing segments in the portfolio, helped by the expected population boom in light of the reversal of the single child policy last year as well as a growing health-conscious middle class in China. Popular international brands like Blackmores, Nature Made and Garden of Life made their debut at the show along with 700 suppliers of health food and supplements, bringing with them popular product lines tailored to the Chinese market.
The Health Industry Summit is organized by Reed Sinopharm, a joint venture between the world’s leading event organizer Reed Exhibitions and China’s leading state-owned medical & pharmaceutical group Sinopharm, ranked number 199 on the latest Fortune 500 list released in July. Its next edition will be held in April 2018 in Shanghai while the 78th China International Medical Equipment Fair (CMEF Autumn 2017) is to take place in Yunnan at the Kunming Dianchi Convention & Exhibition Centre from October 29 to November 1.
Visitor profile
The vast majority of visitors naturally came from China, covering all regions and healthcare sectors. However, there was also a growing segment of international visitors. Topping the list of foreign countries was India with a 20% share of international attendees followed by Korea (15%), Pakistan, Japan, USA, Russia and Germany.
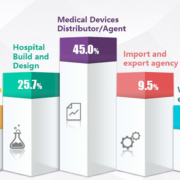
Overall, CMEF visitors spanned the entire medical area – both healthcare and medical device industry. Distributors of medical devices constituted the largest single visitor group with 45% of the total followed by hospital build and design (26%) and rehabilitation centre professionals (see detailed visitor composition chart on previous page).
National pavilions
The international participation is increasing, reflecting the growing importance of China’s healthcare industry. Further adding to the show’s attraction, a large number of national pavilions were featured in a dedicated hall where a constant stream of visitors could view the latest products and technology of companies from countries as diverse as Switzerland, Canada, Taiwan or Germany. For the first time the US and Pakistan had country group exhibits while the Spanish Medical Technology Association (FENIN) led some Spanish companies to make their appearance at the CMEF Spanish pavilion and the German Land of Thuringia organized a regional exhibit for the first time.


MEDICAL FAIR ASIA 2018, is set to continue its growth path with its 12th edition. An expected 1,000 exhibitors from 50 countries and 20 national pavilions will grace the exhibition to be held in Singapore from 29th to 31st August. Visitors will get to source from a comprehensive range of more than 5,000 products ranging from digital health technology, electromedical equipment, rehabilitation supplies to consumables.
There will be a total of 20 National Pavilions and Country Groups, this edition will see debut group participations from Belgium, Brazil, the Netherlands, Iran, Denmark, European Union Business Avenue, Russia, Spain and Qatar, adding to the internationality of the exhibition.
Inaugural Community Care Pavilion
On the show floor, visitors can also expect to see products relating to the current healthcare trends and needs of the Asian region. The debuting Community Care Pavilion, with its keen focus on geriatrics and digital health technology seeks to address the healthcare needs of both the ageing population and the region’s remote population by bringing healthcare beyond traditional healthcare institutions and into the community. Exhibitors have already arranged for product launches to take place during the 3-day period. France Bed Co Ltd will be showcasing their unique powered turning bed. It features an automatic turning support function that prevents users from bed sores. Xiaoniu Health Co Ltd will be unveiling their intelligent sleep machine that can perform both CPAP and AutoCPAP to sleep apnea patients.
Another first on the show floor is the inaugural Start-Up Park. Providing a platform for young and exciting start-ups, the exhibits will feature products that could transform the market in the near future including the latest innovations in big data, and IoT. Australian start-up Rapid Response Revival Research will unveil a prototype of their phone case defibrillator, CellAED, the world’s smallest, lightest and first truly mobile AED (Automatic External Defibrillator) for the very first time.
Conferences and forums
Back by popular demand, the exhibition will play host to the second edition of the MEDICINE + SPORTS Conference. This benchmark event for sports medicine will discuss topics ranging from digital innovations in sports and healthcare, exercise medicine to tailored exercise programmes for patients and athletes. A stellar lineup of speakers including experts Dr. Paul Gastin, Director for the Centre for Sport Research at Deakin University, Mr. Christian Stammel, CEO of WT | Wearable Technologies and Prof. James S. Skinner, Professor Emeritus in the Department of Kinesiology, Indiana University, have been confirmed.
With Start-Ups and SMEs deepening their presence in global business, the exhibition will also host the Medtech SME Workshop. Organized by the first and only regional medical technology association, Asia Pacific Medical Technology Association (APACMed), the workshop will provide small businesses with concise knowledge on clinical trials, product validation, patent laws and many others. Through this workshop, Medtech start-ups and SMEs can learn to navigate processes to develop cost-effective solutions to meet the region’s healthcare needs.
In line with the highlight on Community Care, the exhibition will also feature the first-ever Paradigm Shifts in Healthcare seminar from 30th to 31st August. Leading speakers will discuss the evolution of the healthcare industry while attendees learn how to overcome future challenges as healthcare goes beyond hospitals to the community.
Supported by the Robotic Surgery Society of Singapore, the Medical Innovation & Technology Forum will focus on robotic surgery and discuss how patients evolve from passive healthcare recipients to active value-seekers, encouraging healthcare providers to tap into the latest technological advances to provide more efficient treatment options.
www.medicalfair-thailand.com
Prins Hendrikstraat 1
5611HH Eindhoven
The Netherlands
info@interhospi.com
PanGlobal Media IS not responsible for any error or omission that might occur in the electronic display of product or company data.
