A groundbreaking study published in Nature [1] has reported a significant milestone in the field of human in vitro gametogenesis (IVG), the process of generating mature gametes (sperm and eggs) from pluripotent stem cells in a culture dish.
https://interhospi.com/wp-content/uploads/sites/3/2024/05/gametogenesis-.jpg700700panglobalhttps://interhospi.com/wp-content/uploads/sites/3/2020/06/Component-6-–-1.pngpanglobal2024-05-31 11:10:132024-05-31 11:10:13Major advance in human in vitro gametogenesis achieved
In a groundbreaking move, a panel of leading experts across academia, industry, and government has issued a call to the scientific community to uphold the core values and norms of science amid the revolutionary advances in generative artificial intelligence (AI) through the establishment of a Strategic Council on the Responsible Use of Artificial Intelligence in […]
https://interhospi.com/wp-content/uploads/sites/3/2024/05/AI_evolution.png10241024panglobalhttps://interhospi.com/wp-content/uploads/sites/3/2020/06/Component-6-–-1.pngpanglobal2024-05-22 11:05:322024-05-22 11:25:38Scientific community in the United States calls for safeguarding integrity of science in the age of generative AI
Researchers warn there are too many diseases and pathways of transmission to adapt to climate change
A comprehensive assessment of scientific literature has uncovered empirical evidence that more than 58% of human diseases caused by pathogens, such as dengue, hepatitis, pneumonia, malaria, Zika and more, have been – at some point – aggravated by the hazards of climate change. That alarming finding is the result of a research paper published on August 8 in Nature Climate Change by a team of researchers from the University of Hawaiʻi at Mānoa.
The researchers carried out a systemic search for empirical examples about the impacts of 10 climatic hazards sensitive to greenhouse gas (GHG) emissions on each known human pathogenic disease. These hazards included warming, drought, heatwaves, wildfires, extreme precipitation, floods, storms, sea level rise, ocean biogeochemical change, and land cover change.
Combining two authoritative lists of all known infections and pathogenic diseases that have affected humanity in recorded history, researchers then reviewed more than 70,000 scientific papers for empirical examples about each possible combination of a climatic hazard impacting each of the known diseases.
The research revealed that warming, precipitation, floods, drought, storm, land cover change, ocean climate change, fires, heatwaves and sea level changes were all found to influence diseases triggered by viruses, bacteria, animals, fungi, protozoans, plants and chromists. Pathogenic diseases were primarily transmitted by vectors, although case examples were also found for waterborne, airborne, direct contact and foodborne transmission pathways.
Ultimately, the research found that more than 58% (218 out of 375) of known human pathogenic diseases had been affected at some point, by at least one climatic hazard, via 1,006 unique pathways.
“Given the extensive and pervasive consequences of the COVID 19 pandemic, it was truly scary to discover the massive health vulnerability resulting as a consequence of greenhouse gas emissions,” said Camilo Mora, geography professor in the College of Social Sciences (CSS) and lead author of the study. “There are just too many diseases, and pathways of transmission, for us to think that we can truly adapt to climate change. It highlights the urgent need to reduce greenhouse gas emissions globally.”
Online tool shows link between climate hazard and disease
An interactive web-page showing each connection between a climatic hazard and a disease case was developed by the research team. The tool allows users to query specific hazards, pathways and disease groups, and see the available evidence.
Other key findings include:
Climatic hazards are bringing pathogens closer to people. Numerous climatic hazards are increasing the area and duration of environmental suitability facilitating the spatial and temporal expansion of vectors and pathogens. Warming and precipitation changes, for instance, were associated with range expansion of vectors such as mosquitoes, ticks, fleas, birds and several mammals implicated in outbreaks by viruses, bacteria, animals and protozoans, including dengue, chikungunya, plague, Lyme disease, West Nile virus, Zika, trypanosomiasis, echinococcosis and malaria to name a few.
Climatic hazards are bringing people closer to pathogens. Climatic hazards were also implicated with the forced displacement and migration of people causing or increasing new contacts with pathogens. Heatwaves, for instance, have been associated with rising cases of several waterborne diseases such as Vibrio (a kind of bacteria)-associated infections, primary amoebic meningoencephalitis and gastroenteritis. Storms, floods and sea level rise caused human displacements implicated in cases of leptospirosis, cryptosporidiosis, Lassa fever, giardiasis, gastroenteritis, Legionnaires’ diseases, cholera, salmonellosis, shigellosis, pneumonia, typhoid, hepatitis, respiratory disease and skin diseases among others.
Climatic hazards have enhanced specific aspects of pathogens, including improved climate suitability for reproduction, acceleration of the life cycle, increasing seasons/length of likely exposure, enhancing pathogen vector interactions (for example, by shortening incubations) and increased virulence. For instance, storms, heavy rainfall and floods created stagnant water, increasing breeding and growing grounds for mosquitoes and the array of pathogens that they transmit (for example, leishmaniasis, malaria, Rift Valley fever, yellow fever, St. Louis encephalitis, dengue and West Nile fever). Climatic hazards were also implicated in the increasing capacity of pathogens to cause more severe illness. For example, heatwaves were suggested as a natural selective pressure toward “heat resistant” viruses, whose spillover into human populations results in increased virulence as viruses can better cope with the human body’s main defense, which is fever.
Climatic hazards have also diminished human capacity to cope with pathogens by altering body condition; adding stress from exposure to hazardous conditions; forcing people into unsafe conditions; and damaging infrastructure, forcing exposure to pathogens and/or reducing access to medical care. Drought, for instance, was conducive to poor sanitation responsible for cases of trachoma, chlamydia, cholera, conjunctivitis, Cryptosporidium, diarrheal diseases, dysentery, Escherichia coli, Giardia, Salmonella, scabies and typhoid fever.
Researchers also found that, while the great majority of diseases were aggravated by climatic hazards, 63 out of 286 diseases diseases were diminished by some climatic hazards, although 54 of them were at times also aggravated by other climatic hazards; only nine pathogenic diseases were exclusively diminished by climatic hazards. Warming, for example, appears to have reduced the spread of viral diseases probably related to unsuitable conditions for the virus or because of a stronger immune system in warmer conditions.
“We knew that climate change can affect human pathogenic diseases,” said co-author Kira Webster, CSS geography PhD student. “Yet, as our database grew, we became both fascinated and distressed by the overwhelming number of available case studies that already show how vulnerable we are becoming to our ongoing growing emissions of greenhouse gases.”
https://interhospi.com/wp-content/uploads/sites/3/2022/08/climate-change_1.jpg11601701panglobalhttps://interhospi.com/wp-content/uploads/sites/3/2020/06/Component-6-–-1.pngpanglobal2022-08-10 09:47:562022-08-10 09:50:30Large study shows climate change aggravates more than 58% of all known pathogenic human diseases
Cambridgeshire, UK-based Paragraf, the first company in the world to deliver a scalable approach to graphene electronic device manufacturing, has announced a plan to develop a new generation of graphene-based, in-vitro diagnostic products that will give results within a few minutes.
With the support of a £550,000 Biomedical Catalyst grant award from Innovate UK, Paragraf initiated a two-year programme to develop a proof-of-concept combined PCT (procalcitonin) and CRP (C-reactive protein) test, on a single panel. On March 1 this year Paragraf raised US$60 million in a Series B financing round.
The company is collaborating with the universities of Liverpool, Manchester and Newcastle, Newcastle upon Tyne Hospitals NHS Foundation Trust and Manchester University NHS Foundation Trust (MFT), on the development.
Clinical study of graphene-based PCT/CRP test
A clinical study of the combined PCT/CRP test will be delivered at MFT’s Diagnostics and Technology Accelerator (DiTA) in mid-2023. DiTA aims to address unmet needs, transform patient care and improve efficiency within the NHS, by facilitating the rapid translation and adoption of new innovations into the healthcare system. The project is expected to be completed by the end of May 2024.
Paul Dark, Professor of Critical Care Medicine at The University of Manchester, and Honorary NHS Consultant at Salford Royal, part of Northern Care Alliance NHS Foundation Trust, said: “We expect to show that our proposed acute inflammatory marker test will have the capability to deliver accurate results for emergency patient care within a few minutes, from a small sample of blood. The accuracy of the test is envisaged to be at least comparable with hospital centralised lab-based immunoassay tests which can take hours to provide results back to emergency services.”
Prof. Dark also leads the National Institute for Health and Care Research (NIHR) Manchester Biomedical Research Centre (BRC), Respiratory Non-fungal Infections Programme, which is focused on providing more accurate, rapid diagnosis for patients with severe respiratory infections.
Malcolm Stewart, Paragraf Diagnostics Business Development Director
Antimicrobial stewardship
Malcolm Stewart, Paragraf Diagnostics Business Development Director, said: “This graphene-based diagnostic test is expected to become the first test in the world to give clinicians the ability to identify patients who need an antibiotic treatment within the space of a regular 15-minute clinic appointment. It encourages antimicrobial stewardship by giving clinicians the insight into when not to prescribe antibiotics as the test result differentiates viral from bacterial infections.”
The role of graphene in the in-vitro test
Commenting on the role of graphene in the test, Stewart explained that graphene enhances the test by having the ability to detect very low levels of the target protein (in this case). “Graphene is one of the most conductive substances ever discovered. The almost immediate electrical conductivity change in the graphene when only picogram levels of the target (in this case PCT) are detected is the difference the graphene makes. Simply put, graphene allows us to detect much lower concentrations of target analytes and in single digit minutes than is conventionally possible – and in a piece of equipment that will be handheld in size.
“We can make the graphene into chip-like devices – called graphene field effect transistors (GFETS) – which allow us to detect multiple analytes on one chip, a technique called multiplexing. This first test we are working on will detect two analytes on one chip – PCT and CRP. In future, tests we will be multiplexing more than six analytes on one chip in the cartridge.
“Graphene is also biocompatible meaning that we can deposit samples without having to pre-prepare them. So in this case, for the PCT/CRP test, we will only require a couple of drops of blood directly into the test cartridge. The reduction in pre-analytical errors is vital for tests like this one being used in critical care areas where time to result is important. Once this test is being used in primary care the lack of pre-preparation of the sample makes the test feasible in a GP surgery or even in a patient’s home,” Stewart explained.
Enitan Carrol, Professor of Paediatric Infectious Diseases at the University of Liverpool, reiterated this point: “This technology reduces the time and complexity of sample preparation which, together with its rapid measurement speed, provides clinicians with accurate results in a timeframe that allows immediate decisions to be made on antimicrobial prescribing. This is especially important for the treatment of children and neonates.”
Paragraf
Manufacturing the graphene in-vitro tests
Explaining the manufacturing process, Stewart said: “As we scale up our business, the graphene will be deposited on to larger wafers – 20 or 30cm diameter – in the future. We then make GFETS from the wafers.
“Our process is called MOCVD (metal oxide chemical vapour deposition) and is not unique to us. But the way we do it and the ingredients we use makes it unique. We can make graphene that is contamination free, because or graphene is directly formed on the wafer rather than transferred from another metal like copper in other graphene manufacturing processes.
“We believe we have a technique that is scalable to millions of chips a year when we are manufacturing our chips on 30cm wafers.”
Plans for series of tests for disease biomarkers
Paragraf plans to deliver a series of high sensitivity, rapid tests for disease biomarkers in areas including cardiovascular disease, oncology, and infectious diseases.
The ambition is to develop a comprehensive suite of tests that could be used in almost any environment or healthcare setting. The tests are designed to provide ultra-fast answers to diagnostic challenges and to create a complete diagnostic toolkit at the point of care.
https://interhospi.com/wp-content/uploads/sites/3/2022/07/Paragraf-Diagnostics-Device-Concept_1.jpg9571701panglobalhttps://interhospi.com/wp-content/uploads/sites/3/2020/06/Component-6-–-1.pngpanglobal2022-07-20 11:13:022022-07-20 11:14:28UK company to develop world’s first graphene-based rapid in-vitro diagnostic test
Karen Miga, assistant professor of biomolecular engineering at UC Santa Cruz, co-led the Telomere-to-Telomere (T2T) Consortium, which has released the first complete, gapless assembly of a human genome sequence. (Photo by Carolyn Lagattuta)
The first truly complete sequence of a human genome, covering each chromosome from end to end with no gaps and unprecedented accuracy, is now accessible through the UCSC Genome Browser and is described in six papers published March 31 in Science.
Since the first working draft of a human genome sequence was assembled at UC Santa Cruz in 2000, genomics research has led to enormous advances in our understanding of human biology and disease. Nevertheless, crucial regions accounting for some 8% of the human genome have remained hidden from scientists for over 20 years due to the limitations of DNA sequencing technologies.
“Ever since we had the first draft human genome sequence, determining the exact sequence of complex genomic regions has been challenging,” said Evan Eichler, Ph.D., researcher at the University of Washington School of Medicine and T2T consortium co-chair. “I am thrilled that we got the job done. The complete blueprint is going to revolutionize the way we think about human genomic variation, disease and evolution.”
Telomere-to-Telomere Consortium
The sequencing and analysis were performed by a team of more than 100 people, the so-called Telemere-to-Telomere Consortium, or T2T, named for the telomeres that cap the ends of all chromosomes. T2T was initially set up in 2019 by Karen Miga, assistant professor of biomolecular engineering at UC Santa Cruz, and Adam Phillippy at the National Human Genome Research Institute (NHGRI).
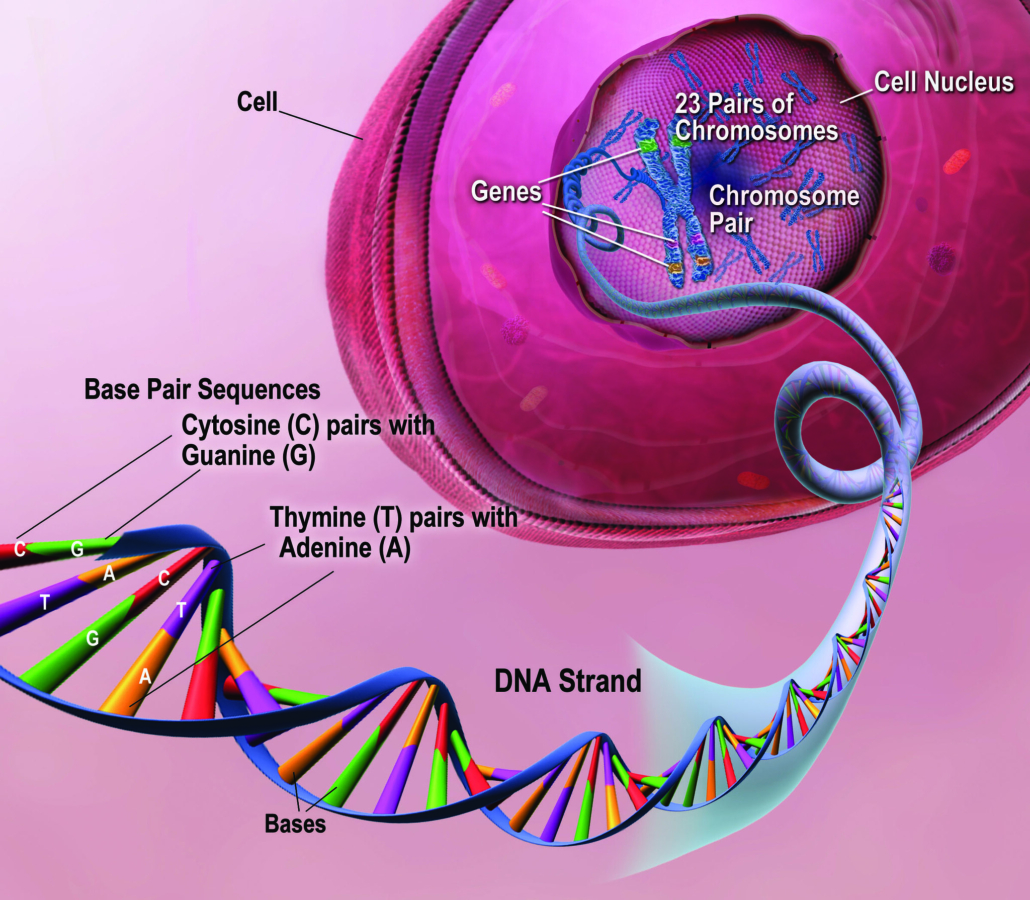
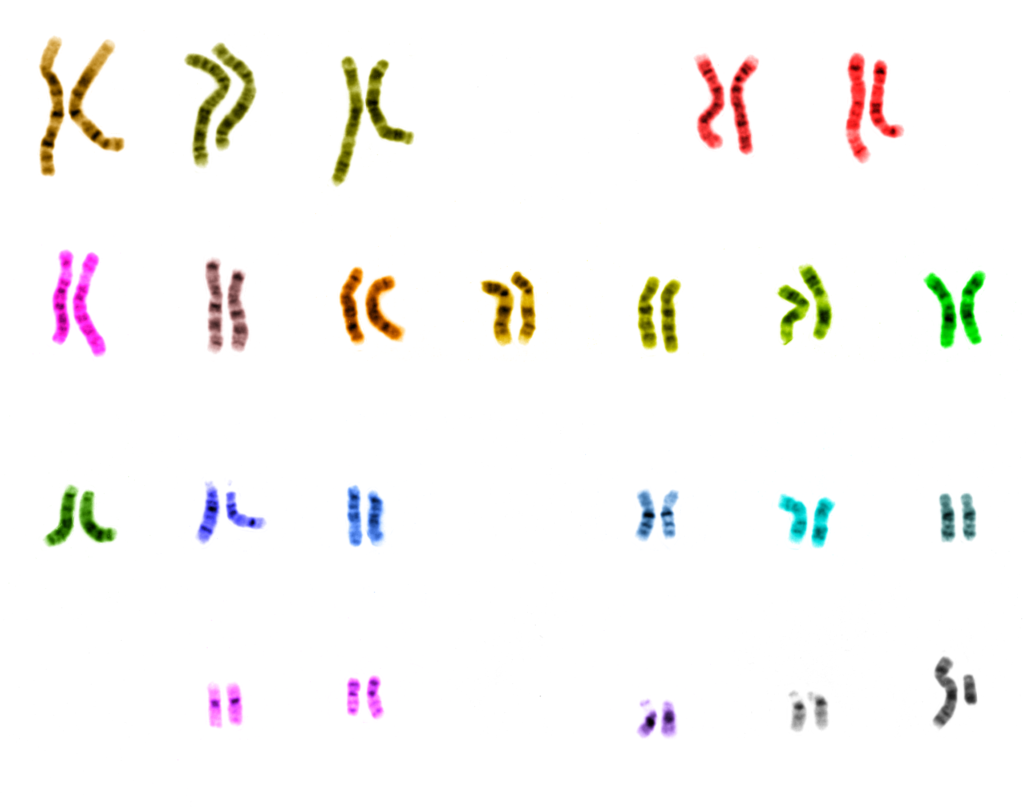
The consortium’s gapless version of all 22 autosomes and the X sex chromosome is composed of 3.055 billion base pairs, the units from which chromosomes and our genes are built, and 19,969 protein-coding genes.
The new reference genome, called T2T-CHM13, adds nearly 200 million base pairs of novel DNA sequences, including 99 genes likely to code for proteins and nearly 2,000 candidate genes that need further study. It also corrects thousands of structural errors in the current reference sequence.
Complete sequence of a Y chromosome
The researchers also released this week the complete sequence of a Y chromosome from a different source, which took nearly as long to assemble as the rest of the genome combined, said Nicolas Altemose, a postdoctoral fellow at the University of California, Berkeley, and a co-author of four new papers about the completed genome. The analysis of this new Y chromosome sequence will appear in a future publication.
“In the future, when someone has their genome sequenced, we will be able to identify all of the variants in their DNA and use that information to better guide their health care,” said Phillippy, one of the leaders of T2T and a senior investigator at NHGRI. “Truly finishing the human genome sequence was like putting on a new pair of glasses. Now that we can clearly see everything, we are one step closer to understanding what it all means.”
The gaps now filled by the new sequence include the entire short arms of five human chromosomes and cover some of the most complex regions of the genome. These include highly repetitive DNA sequences found in and around important chromosomal structures such as the telomeres at the ends of chromosomes and the centromeres that coordinate the separation of replicated chromosomes during cell division.
New discoveries
The new DNA sequences reveal never-before-seen detail about the region around the centromere. Variability within this region may also provide new evidence of how our human ancestors evolved in Africa.
“Uncovering the complete sequence of these formerly missing regions of the genome told us so much about how they’re organized, which was totally unknown for many chromosomes,” said Altemose. “Before, we just had the blurriest picture of what was there, and now it’s crystal clear down to single base pair resolution.”
The new sequence also reveals previously undetected segmental duplications, long stretches of DNA that are duplicated in the genome and are known to play important roles in evolution and disease.
“These parts of the human genome that we haven’t been able to study for 20-plus years are important to our understanding of how the genome works, genetic diseases, and human diversity and evolution,” Miga said.
Many of the newly revealed regions have important functions in the genome even if they do not include active genes.
What they found in and around the centromeres were layers of new sequences overlaying layers of older sequences, as if through evolution new centromere regions have been laid down repeatedly to bind to the kinetochore. The older regions are characterized by more random mutations and deletions, indicating they’re no longer used by the cell. The newer sequences where the kinetochore binds are much less variable, and also less methylated. The addition of a methyl group is an epigenetic tag that tends to silence genes.
All of the layers in and around the centromere are composed of repetitive lengths of DNA, based on a unit about 171 base pairs long, which is roughly the length of DNA that wraps around a group of proteins to form a nucleosome, keeping the DNA packaged and compact. These 171 base pair units form even larger repeat structures that are duplicated many times in tandem, building up a large region of repetitive sequences around the centromere.
DNA sequences around the centromere could also be used to trace human lineages back to our common ape ancestors, he noted.
“As you move away from the site of the active centromere, you get more and more degraded sequence, to the point where if you go out to the furthest shores of this sea of repetitive sequences, you start to see the ancient centromere that, perhaps, our distant primate ancestors used to bind to the kinetochore,” Altemose said. “It’s almost like layers of fossils.”
Seeing the whole genome as a complete system for the first time
“There is a profound advantage to seeing the whole genome as a complete system. It puts us in a position to unravel how that system works,” said David Haussler, director of the UC Santa Cruz Genomics Institute. “We’ve gotten an enormous understanding of human biology and disease from having roughly 90 percent of the human genome, but there were many important aspects that lay hidden, out of view of science, because we did not have the technology to read those portions of the genome. Now we can stand at the top of the mountain and see all of the landscape below and get a complete picture of our human genetic heritage.”
The T2T genome sequence, representing the finished CHM13 genome plus the recently finished T2T Y chromosome (CHM13 includes an X but not a Y chromosome), is now a new reference genome in the UCSC Genome Browser. The T2T sequence is fully annotated in the browser, providing an efficient way for scientists to access and visualize a wealth of information associated with genes and other elements of the genome.
“We wanted to put the information out in a way that is accessible and familiar to researchers so they can begin to build on it and use all the tools and resources the browser provides,” Miga explained.
Genome Reference Consortium
The new T2T reference genome will complement the standard human reference genome, known as Genome Reference Consortium build 38 (GRCh38), which had its origins in the publicly funded Human Genome Project and has been continually updated since the first draft in 2000.
“We’re adding a second complete genome, and then there will be more,” explained Haussler. “The next phase is to think about the reference for humanity’s genome as not being a single genome sequence. This is a profound transition, the harbinger of a new era in which we will eventually capture human diversity in an unbiased way.”
Human Pangenome Reference Consortium
The T2T Consortium has now joined with the Human Pangenome Reference Consortium, which aims to create a new “human pangenome reference” based on the complete genome sequences of 350 individuals.
“Pangenomics is about capturing the diversity of the human population, and it’s also about ensuring we’ve captured the whole genome properly,” said Benedict Paten, associate professor of biomolecular engineering at UCSC’s Baskin School of Engineering, a coauthor of the T2T papers, and a leader of the pangenomics effort. “Without having a map of these difficult-to-sequence regions of the genome across multiple individuals, then we’re missing a huge amount of the variation present in our population. T2T sets us up to look across hundreds of genomes from telomere to telomere. It’s going to be great!”
The standard reference genome (GRCh38) does not represent any one individual but was assembled from multiple donors. Merging them into one linear sequence created artificial structures in the sequence. The Human Pangenome Project will make it possible to compare newly sequenced genomes to multiple complete genomes representing a range of human ancestries.
More accurate assessments of genetic variants
An important outcome of the new T2T sequence is enabling more accurate assessments of genetic variants. When human genomes are sequenced for clinical studies to understand the role of genetic variants in disease or to study genetic diversity within and between human populations, they are nearly always analyzed by aligning the sequencing results with the reference genome for comparison. The T2T variant team documented major improvements in identifying and interpreting genetic variants using the new T2T sequence compared to the standard human reference genome.
“The new human genome is incredibly accurate at the base level, allowing us to flag hundreds of thousands of variants that had been misinterpreted by mapping them to the standard reference. Many of these new variants are in genes known to contribute to disease. We can now spot those because we have a more complete and accurate reference genome,” Miga said.
Miga’s research has focused on satellite DNA, the long stretches of repetitive DNA sequences found mostly in and around telomeres and centromeres. The centromeres separate each chromosome into a short arm and a long arm and hold duplicated chromosomes together prior to cell division.
“The centromeres play a critical role in how chromosomes segregate properly during cell division, and we’ve known for some time now that they are misregulated in all kinds of human diseases. But we’ve never been able to study them at the sequence level,” Miga said. “By far the largest portion of new sequences added to the reference are centromere satellite DNAs. For the first time, we can study ‘base-by-base’ the sequences that define the centromere and can start to understand how it works.”
Long-read sequencing a game changer
The T2T’s success is due to improved techniques for sequencing long stretches of DNA at once, which helps when determining the order of highly repetitive stretches of DNA. Among these are PacBio’s HiFi sequencing, which can read lengths of more than 20,000 base pairs with high accuracy. Technology developed by Oxford Nanopore Technologies, on the other hand, can read up to several million base pairs in sequence, though with less fidelity. For comparison, so-called next-generation sequencing by Illumina is limited to hundreds of base pairs.
“These new long-read DNA sequencing technologies are just incredible; they’re such game changers, not only for this repetitive DNA world, but because they allow you to sequence single long molecules of DNA,” Altemose said. “You can begin to ask questions at a level of resolution that just wasn’t possible before, not even with short-read sequencing methods.”
———
Karen Miga
Miga is a co-corresponding author of the main Science paper along with Adam Phillippy at NHGRI and Evan Eichler at the University of Washington:
https://interhospi.com/wp-content/uploads/sites/3/2022/04/man-2125123-e1680870804302.png7511000panglobalhttps://interhospi.com/wp-content/uploads/sites/3/2020/06/Component-6-–-1.pngpanglobal2022-04-01 14:48:592022-04-01 15:07:27In major breakthrough, scientists complete first gapless sequence of a human genome, reveal hidden regions
Harald Huber, Global VP for Product and Category Management at Pentax Medical
International Hospital’s Twan Heesakkers speaks to Harald Huber, Global VP for Product and Category Management at PENTAX Medical, about the company’s new single-use bronchoscope, what they are focusing on this year and the ‘Power of Choice’.
Twan Heesakkers: What new products are you bringing to the market this year? Harald Huber: This year we will bring a couple of new things to the market. We would like to put more emphasis on the [PENTAX Medical] ONE Pulmo, by creating more public awareness of the product. The ONE Pulmo is a single-use bronchoscope, our first product in the single-use area. We also have the PlasmaTYPHOON+, our unique solution for endoscope drying and storage, which we will also push forward. Furthermore, we are working very hard on providing innovative solutions, instead of following the traditional way the endoscope business was set up, which was more into products and endoscopic processors. We want to bring our way of thinking forward, which is more focussed on developing solutions rather than pure product business. So we want to interconnect these things, for example the PlasmaTYPHOON+ is part of our hygiene commitment. We are calling this the ‘Power of Choice’. This Power of Choice will also apply to our single-use endoscopes and has a compelling advantage for our customers. The idea behind ‘Power of Choice’ is that we do not want to dictate to our customers what kind of procedure they have to do. We want to allow them the highest possible freedom to pick the right equipment for their procedure. That’s why we want to offer as many solutions as possible in different areas and move away from the traditional thinking about products.
The PENTAX Medical ONE Pulmo single-use bronchoscope.
TH: You mentioned the single-use bronchoscope – the PENTAX Medical ONE Pulmo for which you received the CE mark last year? Can you tell us a little more about this product; what sets it apart from similar competitors’ products?
HH: When we came up with this solution we thought, ‘if we, as PENTAX Medical, come up with a single-use bronchoscope how will it be different?’ As you know, our company produces reusable products and everybody will ask, why are we coming up with a single-use bronchoscope? And that’s again in line with our idea of providing the Power of Choice. So the difference, I think, to other single-use bronchoscopes that you see on the market is that this is probably the first one that is purely developed by an endoscope company. So, with our expertise in image development we were able to develop a camera in such a way that on one side its single-use, while on the other side it can provide comparable image quality to our reusable scopes. This is kind of the red line throughout the whole design process and differentiates us from the competition. It also continues with the design of the control body, with the handle actually. We want to provide a real Power of Choice. Doctors should not have to care if they use the single-use scope or the reusable one. They want to have the same familiar touch and feel that they are used to when doing an endoscopy procedure. That’s why we mimic the reusable scope, so it has the same properties of a reusable scope, and we develop it in such a way that it can be offered as a single-use solution.
The PENTAX Medical ONE Pulmo is a single-use bronchoscope with superior suction power and HD image quality. The sterile-packed scopes are ready to use. Manoeuvrability and device insertion are easy and intuitive, creating a seamless user experience.
TH: Besides offering the ‘Power of Choice’, what other reasons are behind PENTAX Medical choosing to develop a single-use disposable bronchoscope?
HH: ‘Choice’ is an important factor as to why we did this. The other thing is that there is of course concern about contamination. There are special patient populations where it definitely makes sense to go for a single-use scope. We know that it does not make sense for all patient populations. Also, you have the sustainability factor, you have the cost of cleaning, pricing of the product, etc. There are multiple factors which tell you that single-use doesn’t make sense for all patients. However, it makes sense for a certain population – for example patients who are immunocompromised. Imagine somebody who has a very high health risk if somehow cross infected with a germ that is transmitted during the procedure. For this patient do we go with a reusable cope or will we take a single-use scope? And that’s the doctor’s decision, but what we want to make sure as a provider/manufacturer that there is little difference in the choice of scope so the same quality of care can be provided to the patient. Because if you do it the other way around and you are a pure single-use provider you cannot offer this choice.
The PENTAX Medical Video Duodenoscopes ED32-i10 and ED34-i10T2 combine a sterile disposable elevator cap (DEC™) for single-patient use and simple disposal that advances cleaning capability of the duodenoscope to help reduce the risk of cross-contamination and improve patient care with High-Definition image quality for detailed endoscopic visualization during ERCP procedures.
Distal end of the PENTAX Medical Video Duodenoscope ED32-i10
TH: PENTAX Medical is leading the collaborative i-scan imaging processing project. Can you explain what this project is about and the purpose of it.
HH: “i-scan is one part of our general solutions approach. For i-scan there are different modalities which support doctors in each step of the diagnostic process. These i-scan modalities include SE – or Surface Enhancing mode – that improves detection, particularly of the shadowed parts of the lesion. There is TE – or Tone Enhancement – which helps in the characterization of the lesion by amplifying the colours so the doctors understand better what they are seeing and can make an informed medical decision. Then we have OE – or Optical Enhancement – an optical filter which helps in demarcation, to understand the actual size of the lesion in the macule that the doctor sees.
This is an example of how we support doctors each step of the way and that’s part of our solution-driven thinking. We are also involved with many physicians for the i-scan project all across Europe and some parts from the US. They add to the project by sharing their insights on how they can benefit from i-scan in their medical procedures. We also use this as part of our learning initiative. Whenever they have tricky images they have identified, they bring them to a forum where they can be discussed.
TH: PENTAX Medical has developed their own data management and software solutions for their medical imaging devices. Can you tell us more about these solutions?
HH: We are deprioritizing data management and hospital software solutions. We are now more focussed on a solutions approach by combining our products and services.
TH: PENTAX Medical’s latest image and video processor is the Optivista Plus. I understand it can also be used as an educational platform with its “TwinMode” setting. Can you tell us more about this device?
HH: The TwinMode is an interesting feature! As part of the educational setting, it is possible to show a previously recorded image on the screen so the doctor, or the students in training, can compare these images with the current ones they are seeing. So, for example with the i-scan project, images enhanced with one of the modalities can be compared to the same image without any enhancements. That’s how students learn when they can compare.
TH: What else is in the pipeline for PENTAX Medical? HH: Our focus is set in the hygiene cosmos, where we have initiatives such as Power of Choice. We also have our World of Intelligence initiative that is focussed on the digital arena, like AI, which supports our solutions-driven approach. We ask the question, what kind of solution can we provide with our different products if you, the customer, combine them together. We have the processors and we have the scopes, we have the single-use scope, we have the semi disposable scopes, we have different image modalities which can be used in different combinations in order to provide the right solution for their particular case. So all that comes together with us being able to provide this choice for doctors.
https://interhospi.com/wp-content/uploads/sites/3/2022/03/harald_huber.jpg8741566panglobalhttps://interhospi.com/wp-content/uploads/sites/3/2020/06/Component-6-–-1.pngpanglobal2022-03-15 13:14:012022-03-17 07:42:47Interview: International Hospital speaks to PENTAX Medical about their new focus on ‘Power of Choice’
The IHF stands with hospitals during conflict, calls on members to provide support
The situation in Ukraine is a major concern for all of us, and the escalation of violence that has been reported on many different channels is alarming.
On 25 February, we released a message of solidarity with the people and the healthcare community in Ukraine.
The escalation of violence impacting hospitals and healthcare personnel is being reported by many authorities including:
UN Office for the Coordination of Humanitarian Affairs (UNOCHA) (here).
International Committee of the Red Cross (ICRC) (here).
Attacks on hospitals, healthcare workers, and ambulances are not acceptable. No matter the context. No matter the reasons. It is a violation of International Humanitarian Law, and we firmly stand against it.
Many international organizations and local actors are working hard, both inside Ukraine and in the neighbouring countries, such as Poland, Hungary, Slovakia, Moldova, and Romania to support refugees, mainly women and children. The UN Refugee Agency (UNHCR) has issued an alert that the number of refugees could reach 4 million rapidly.
IHF Members want to help, but the Ukrainians have limited logistical capacity to manage donations. We are recommending to the IHF community to get involved (either with financial or supplies support) through organizations acting in the field in neighbouring countries, or to the headquarters of these organizations. These trusted organizations have the capacity to redistribute the donations in a strategic manner.
Many organizations are providing emergency assistance in the region. The IHF would suggest supporting the following:
There are also initiatives that our members and partners have shared with us that we believe you will be interested to discover and support. For example:
The Polish Hospital Federation is cooperating with the Polish Medical Mission (PMM) to provide direct support to the hospitals in Ukraine, as well as in the Polish hospitals located near the Ukraine border (read more here).
Direct financial donations can be made via the PMM website.
Teladoc Health is supporting hospitals in Ukraine through the Ukrainian Government (offering technology and doctors) and is helping refugees in Poland by providing virtual medical care.
If you are a healthcare professional who wants to volunteer, or if you want more information, you can contact Rafael Gotsens, International Medical Director, Teladoc Health, Inc. (rgotsens@teladochealth.com).
https://interhospi.com/wp-content/uploads/sites/3/2022/03/IHF-logo-copy.jpg450450panglobalhttps://interhospi.com/wp-content/uploads/sites/3/2020/06/Component-6-–-1.pngpanglobal2022-03-14 10:43:532022-03-14 10:43:53The International Hospital Federation issues statement in support of Ukraine
As vaccine nationalism and inequitable distribution continue to plague the global rollout of COVID-19 vaccines, epidemiologists from leading academic institutes around world have issued a stark warning that so-called ‘variants of concern’ to SARS-CoV-2, the virus that causes COVID-19, could render current vaccines ineffective in less than a year. Callan Emery reports.
https://interhospi.com/wp-content/uploads/sites/3/2021/05/1_FEATURED_ARTICLE.jpg13541000panglobalhttps://interhospi.com/wp-content/uploads/sites/3/2020/06/Component-6-–-1.pngpanglobal2021-05-06 12:53:072021-05-19 11:52:05We need a people’s vaccine
A study published in the Journal of Digital Imaging (2019) [1] looked at whether Artificial Intelligence (AI)-based, computer-aided detection (CAD) software can be used to reduce false positives per image (FPPI) on mammograms as compared to an FDA-approved conventional CAD. The study showed a 69% decrease in FPPI which, the researchers said, could also potentially […]
https://interhospi.com/wp-content/uploads/sites/3/2021/02/1_FEATURED_ARTICLE.jpg135410003wmediahttps://interhospi.com/wp-content/uploads/sites/3/2020/06/Component-6-–-1.png3wmedia2021-02-26 10:56:272021-03-01 11:35:49Reducing costs, improving outcomes with AI in a radiology practice
Bacteria that develop resistance to antibiotic drugs – superbugs – pose a major global health threat to humanity. In a concerted effort to stave off this threat, several global programmes have been established and numerous new research initiatives are being carried out. Whether they are successful is yet to be seen. International Hospital reports.
Antimicrobial or antibiotic resistance is a major emerging global health threat which continues to escalate around the world. In the EU it is responsible for around 33,000 deaths each year according to the European Commission [1] and is estimated to cost the EU EUR 1.5 billion per year in healthcare costs and productivity losses.
In the United States, the Centers for Disease Control and Prevention (CDC) estimates that more than 2.8 million antibiotic-resistant infections occur in the country each year, and more than 35,000 people die as a result [2].
In the CDC’s 2019 Antimicrobial Resistance Threats Report, Robert R. Redfield, M.D., Director of the CDC, emphasises that we should stop referring to a coming post-antibiotic era. “It’s already here,” he says. “You and I are living in a time when some miracle drugs no longer perform miracles and families are being ripped apart by a microscopic enemy. The time for action is now and we can be part of the solution.”
So, what exactly is antimicrobial resistance (AMR)? Simply put, antimicrobial resistance occurs when microorganisms – such as bacteria, viruses, fungi, protozoa and helminths (worm-like parasites) – mutate or develop a resistance gene when they are exposed to antimicrobial drugs, such as antibiotics, antifungals, antivirals, antimalarials, and antihelminthics. As a result, the drugs become ineffective and infections persist in the body, increasing the risk of morbidity and mortality as well as the spread of the disease to others.
The issue is of such global importance that a political declaration was endorsed by Heads of State at the United Nations General Assembly in New York in September 2016 signalling the world’s commitment to taking a broad, coordinated approach to address the root causes of antimicrobial resistance across multiple sectors, especially human health, animal health and agriculture.
In 2015, the World Health Organization (WHO) established the Global Antimicrobial Resistance and Use Surveillance System (GLASS) [3]. The system calls on countries to monitor and report on antibiotic resistance. The WHO noted in a report published June 1 this year, that in the past three years, participation has grown exponentially. GLASS now aggregates data from more than 64,000 surveillance sites with more than 2 million patients enrolled from 66 countries across the world. In 2018 the number of surveillance sites was 729 across 22 countries.
Hanan Balkhy, Assistant Director-General for antimicrobial resistance at WHO, explained: “The enormous expansion of countries, facilities and patients covered by the new AMR surveillance system allows us to better document the emerging public health threat of AMR.”
On the back of this data, the Organization notes that high rates of resistance among antimicrobials frequently used to treat common infections, such as urinary tract infections or some forms of diarrhoea, indicate that the world is running out of effective ways to tackle these diseases. For instance, the rate of resistance to ciprofloxacin, an antimicrobial frequently used to treat urinary tract infections, varied from 8.4% to 92.9% in 33 reporting countries.
In addition, the WHO expressed concern that the trend will further be fuelled by the inappropriate use of antibiotics during the COVID-19 pandemic. The Organization points out that evidence shows that only a small proportion of COVID-19 patients need antibiotics to treat subsequent bacterial infections and, as such, has issued guidance [4] not to provide antibiotic therapy or prophylaxis to patients with mild COVID-19 or to patients with suspected or confirmed moderate COVID-19 illness unless there is a clinical indication to do so. Solutions
What can be done to counter AMR? Although antimicrobial resistance occurs naturally over time, usually through genetic changes, there are a number of countermeasures. Primarily, healthcare practitioners should reduce the misuse and overuse of antimicrobials which are accelerating AMR. The WHO notes, for example, that in many places, antibiotics are overused and misused in people and animals, and often given without professional oversight. Examples of misuse include when they are taken by people with viral infections like colds and flu, and when they are given as growth promoters in animals or used to prevent diseases in healthy animals.
CDC’s 2019 Antimicrobial Resistant Threats Report
The CDC’s 2019 AR Threats Report lists 18 antibiotic-resistant bacteria and fungi in three categories based on the level of concern to human health – urgent, serious, and concerning. The ‘urgent’ list includes the following five threats: Carbapenem-resistant Acinetobacter Carbapenem-resistant Acinetobacter cause pneumonia and wound, bloodstream, and urinary tract infections. Nearly all these infections happen in patients who recently received care in a healthcare facility. They are estimated to have caused 700 deaths in the US in 2017. Candida auris C. auris is an emerging multidrug-resistant yeast. It can cause severe infections and spreads easily between hospitalized patients and nursing home residents. Clostridioides difficile C. difficile causes life-threatening diarrhoea and colitis (an inflammation of the colon), mostly in people who have had both recent medical care and antibiotics. Estimated death per year in the US: 12,800. Carbapenem-resistant Enterobacteriaceae (CRE) CRE are a major concern for patients in healthcare facilities. Some Enterobacteriaceae are resistant to nearly all antibiotics, leaving more toxic or less effective treatment options. Estimated deaths in the US in 2017: 1,100. Drug-resistant Neisseria gonorrhoeae N. gonorrhoeae causes the sexually transmitted disease gonorrhoeae that can result in life-threatening ectopic pregnancy and infertility, and can increase the risk of getting and giving HIV.
See the report for the complete list. https://www.cdc.gov/drugresistance/pdf/threats-report/2019-ar-threats-report-508.pdf
https://interhospi.com/wp-content/uploads/sites/3/2020/06/logo-footer.png442003wmediahttps://interhospi.com/wp-content/uploads/sites/3/2020/06/Component-6-–-1.png3wmedia2020-08-26 14:35:292020-08-26 14:35:31Superbugs and failing drugs
We may ask you to place cookies on your device. We use cookies to let us know when you visit our websites, how you interact with us, to enrich your user experience and to customise your relationship with our website.
Click on the different sections for more information. You can also change some of your preferences. Please note that blocking some types of cookies may affect your experience on our websites and the services we can provide.
Essential Website Cookies
These cookies are strictly necessary to provide you with services available through our website and to use some of its features.
Because these cookies are strictly necessary to provide the website, refusing them will affect the functioning of our site. You can always block or delete cookies by changing your browser settings and block all cookies on this website forcibly. But this will always ask you to accept/refuse cookies when you visit our site again.
We fully respect if you want to refuse cookies, but to avoid asking you each time again to kindly allow us to store a cookie for that purpose. You are always free to unsubscribe or other cookies to get a better experience. If you refuse cookies, we will delete all cookies set in our domain.
We provide you with a list of cookies stored on your computer in our domain, so that you can check what we have stored. For security reasons, we cannot display or modify cookies from other domains. You can check these in your browser's security settings.
.
Google Analytics Cookies
These cookies collect information that is used in aggregate form to help us understand how our website is used or how effective our marketing campaigns are, or to help us customise our website and application for you to improve your experience.
If you do not want us to track your visit to our site, you can disable this in your browser here:
.
Other external services
We also use various external services such as Google Webfonts, Google Maps and external video providers. Since these providers may collect personal data such as your IP address, you can block them here. Please note that this may significantly reduce the functionality and appearance of our site. Changes will only be effective once you reload the page
Google Webfont Settings:
Google Maps Settings:
Google reCaptcha settings:
Vimeo and Youtube videos embedding:
.
Privacy Beleid
U kunt meer lezen over onze cookies en privacy-instellingen op onze Privacybeleid-pagina.

 WPI-ASHBi/Kyoto University
WPI-ASHBi/Kyoto University