
Ultrasound and imaging of the musculoskeletal system
In the interviews published in International Hospital we focus on a particular field of expertise to find out about the current developments. We spoke to Dr Jean-Louis Brasseur, consultant at Piti

In the interviews published in International Hospital we focus on a particular field of expertise to find out about the current developments. We spoke to Dr Jean-Louis Brasseur, consultant at Piti
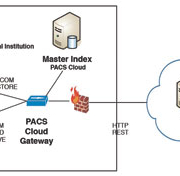
The amount of diagnostic imaging procedures has continuously increased over the last decade and this trend will persist over the coming years. Cloud computing is an emerging solution that promises high scalability of infrastructures, software and applications. This poses the question whether it is advisable that a Picture Archive and Communication System migrates to the Cloud or not.
by Lu

The explosive growth in data generated by healthcare organisations has to be managed. Some available solutions that meet the requirements of clinical imaging are presented here which maximise IT uptime and minimise IT staff shortages issues, as well as creating more business value and facilitating cost savings.
Everyone is talking about cloud computing, yet if ten separate IT professionals were asked to define it, there might well be ten completely different definitions. To date, possibly the clearest and most comprehensive definition has been provided by the National Institute of Standards and Technology (NIST). It describes it as:
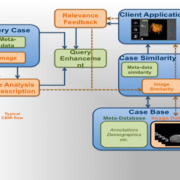
Picture Archiving and Communication Systems (PACS) enable efficient digital storage and remote communication of images from multiple medical imaging modalities. While PACS have significantly reduced the physical overload of managing medical image archives, they have also introduced a challenging mental overload to the radiologist in interpreting imaging findings. In this brief communication, we make the point that content-based retrieval approaches for decision support, such as the CaReRa project, can ease the radiological interpretation process.
by Dr Ceyhun Burak Akg
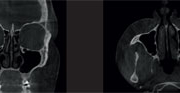
Diagnostic imaging of the ear, nose and throat (ENT) area has traditionally been carried out with medical CT, MRI and standard radiography. Nowadays there is a transition towards using more cone-beam computed tomography (CBCT) for certain diagnostic tasks in these areas. The successful introduction of a CBCT system for ENT applications, in addition to applications in the dental field where the method already plays a major role, is described here.
by Dr Jorma J
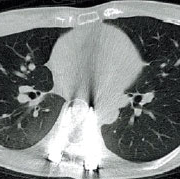
The rapidly developing field of interventional oncology is testimony to many new technological developments t in the fight against cancer. Multiple new, minimally invasive technologies have emerged over the last few years, offering patients new therapeutic options especially when conventional therapy fails or is deemed unsuitable. In addition, many new technologies have been developed for imaging cancer, especially functional imaging which offers patients the chance to verify early tumour response and early recurrence
by Prof. Dr Thomas J. Vogl and Dr Mark Tan
Emerging role of the radiologist
Radiologists are often thought to play a passive role when it comes to patient care. The radiologist evaluates the radiographic imaging or performs an interventional procedure in accordance with the clinician
Inter-shift handover in the emergency department (ED) has long been identified as a high risk undertaking when it comes to patient safety. At the Graduate Entry Medical School, University of Limerick, the Lean process has been instrumental in helping to find solutions to current challenges in the emergency department.
by Dr Rosa McNamara and Dr Fergal Cummins
Patient handover is the term used to describe the act of transferring care from one healthcare professional to another. The terms ‘patient handoff’, ‘sign-out’ and ‘transitions of care’ are also used to describe this process. The act of handover has been identified as a risk in terms of patient safety, and has been described as a point where safety often fails first [1]. Faulty handoffs have been specifically implicated in 24% of malpractice claims in the Emergency Department [2].
Poor handover is associated with a number of adverse effects such as having to re-examine or re-interview the patient [4] inaccurate clinical assessment, delayed diagnosis, delayed investigation, medication errors, inconsistent or incorrect results translation, duplication of results, increased length of stay in hospital, increased in-hospital complications, and decreased patient satisfaction [3].
In a large prospective study, 914 patients were observed during 60 handovers in three metropolitan EDs [4]. They found that information was lacking in 15.4% of handovers, such as information on management, investigations or disposition. In these cases, 56.9% resulted in an adverse event for the doctor and 30.3% for the patient. Adverse events for the doctor included duplication of work, for example, re-interviewing or re-examination of the patient.
Although scripting or verbal standardisation has been recommended [5], a satisfactory and reliable tool to improve quality of ED handover remains elusive [6,7].
Recently, the American College of Emergency Physicians published a document detailing the current evidence regarding ED handoff, providing, a list of suggested handover quality measures, amongst other recommendations [8].
The Department of Emergency Medicine at the University Hospital, Limerick, sees approximately 60 000 patients per year. By applying these standards, it became clear that existing handover processes were inefficient and potentially posed a threat to patient safety. Formal documentation of handover on written notes was low. Only 6% of notes − on audit − met the standards suggested by the American College of Emergency Physicians.
During the auditing of the handover process, it became very clear that there was duplication of history taking and patient examination. After action group meetings within the ED between senior and junior medical staff, an initial decision was made to introduce a formal board round, and new policies were brought in to ensure handover was recorded using the electronic patient tracker programme (MAXIMS
A Mass Casualty Incident (MCI) results in many casualties that require extraordinary care which has to be completely managed with the resources available within the area where the event occurred. In such a crisis situation, hospitals are the centre of medical response and an integral part of the total medical capacity of the community affected. Hospitals must be ready to accommodate a sudden influx of patients requiring care around the clock, every day of the year.
by Prof. F. Della Corte, Dr D. Colombo and Dr P. L. Ingrassia
Given this scenario, many pertinent questions arise. Are we ready to cope with such scenarios? How prepared are we? How long do we need to be ready before an incident occurs that could lead to a great many acutely injured and/or ill patients?
To better understand the role of preparedness, it is necessary to define the concept of ‘surge’, which is the sizeable increase in demand for resources compared with a baseline demand. In healthcare, surge leads to a huge rise in demand for medical and public health resources [1]. Surge also describes the limits of a healthcare system to suddenly expand its ability beyond normal services to meet the bigger demand for qualified medical staff and services during a major event.
The aim is to take care of the maximum number of victims and reduce physical sequelae and mental traumas. In theory, a surge system has the following components: supplies, personnel, physical spaces, and management infrastructure, often referenced to as the 3S (stuff, staff and system) [2,3]. In other words, the hospital surge capacity is based on critical benchmarks and sentinel indicators that are related to its various components. These benchmarks and indicators allow the hospital to better estimate the immediate needs in case of a large influx of patients [4].
Tools to train for a disaster
Simulation, using table-top, electronic and full-scale exercises of MCIs are recognised as useful methods to assess performance, test plans, and investigate the efficiency of surge capacity. To help with these tasks, our research groups collaborated to develop two different simulation tools to be used for education and training in pre- and in-hospital preparedness. They are the Interactive Simulation Exercises of Emergencies (ISEE)

Prins Hendrikstraat 1
5611HH Eindhoven
The Netherlands
info@interhospi.com
PanGlobal Media IS not responsible for any error or omission that might occur in the electronic display of product or company data.
