
Increased embryo viability during In Vitro Fertilization
Fertility in women decreases rapidly after the age of 35 and even more so after 40. Official figures show that women in their early forties have only a 13% chance of conceiving per in vitro fertilization (IVF) treatment. Thus, fertility experts are continuously looking for ways to improve the chances of pregnancy before and during the IVF cycle. At the Newcastle Fertility Centre at Life (part of the Newcastle Hospitals NHS Foundation Trust) a team led by Professor Mary Herbert developed a novel system for processing embryos during IVT treatment. Professor Herbert talked to IHE about this new system, and how chances of pregnancy have grown significantly as a result.
Building on traditional methods
Traditionally, in IVF procedures, processing involves the use of open-fronted microbiological (Class II) safety cabinets and stand-alone incubation chambers. Embryos are cultured in a controlled environment. However, as development has to be checked regularly under a microscope, the embryo has to be removed from this environment and exposed to ambient conditions which may result in deviations from physiological temperature and pH which could alter cell physiology by disrupting fundamental cellular processes such as protein folding, enzyme activity, and assembly of the cytoskeleton.
Thus, to counter the risk of cellular stress, the Newcastle team developed a totally enclosed system of interlinked isolator-based work stations designed to maintain oocytes and embryos in a physiological environment throughout the IVF process. By doing so, the environment is controlled and monitored from the moment oocytes are being harvested from the ovary until embryos are transferred to the uterus.
Simple yet effective
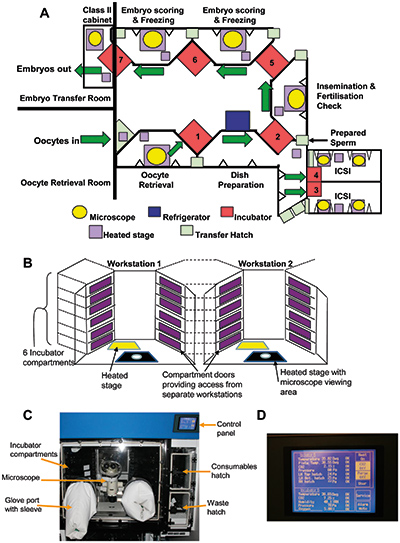
Each system entails a chain of pressure-sealed, enclosed work stations with integrated incubators and built-in microscopes [Figure 1A] which monitors the blastocyst stage, significantly improving fertilization success rates.
The chain of work stations was configured to link adjacent patient treatment rooms in which oocyte retrievals and embryo transfers are conducted [Figure 1A]. To avoid removing embryos from the enclosed system, double-doored incubation chambers were introduced. These chambers can then be accessed from adjacent work stations. As a result, oocytes and embryos can remain in an enclosed environment throughout the process
