

Anemia in pregnancy is one of the most common medical problems pregnant women encounter in both low and high income countries. It affects some 32 million pregnant women worldwide each year and is characterized by a lack of red blood cells. Women with severe anemia will have a blood count of less than 70 grams of hemoglobin per litre of blood. It is a dangerous condition and if not prevented or treated correctly can lead to maternal death.
Highlighting the danger, an international study published in May this year, shows that women with severe anemia during pregnancy or up to seven days after delivery have double the risk of dying compared to those who don’t suffer from the condition.
Previous studies had suggested that anemia was strongly associated with maternal death, but they were not clear due to the influence of other clinical factors. This study – the largest of its kind – is the first to control factors that can influence the development of anemia in pregnancy (such as blood loss or malaria infection) and which may have skewed the results of previous studies.
The researchers emphasize that clinicians, policy makers and healthcare professionals should now focus their attention on preventing anemia, using a multifaceted approach, and not just hope that iron tablets will solve the problem.
Although anemia is a readily treatable condition, the existing approaches have so far not been able to tackle the problem, say the researchers who published their study in the MAY/ JUNE 2018 issue of The Lancet Global Health.
For the study they looked at World Health Organization data on 312,281 pregnancies in 29 countries around the world. The study results show that, when all known contributing factors are controlled for, the odds of maternal death are doubled in mothers with severe anemia.
Importantly, the relationship between severe anemia and the increased risk of maternal death is seen in different geographical areas and, by using different statistical approaches, the researchers are able to show an independent relationship between severe anemia and maternal death does exist.
Prior to this research, the absence of robust data showing evidence of the relationship between severe anemia and maternal mortality has led to a relatively low prioritization of anemia as an important condition in its own right. This new research will hopefully motivate health policy makers to sharpen their focus on the prevention of anemia during pregnancy when they shape new policy on the condition.

Interventional radiology is a subspecialty providing minimally invasive image-guided diagnosis and treatment of disease. The number of procedures performed by interventional radiologists is extensive, ranging from the purely diagnostic such as angiography and cholangiography to the therapeutic, covering vascular and ablative applications. In recent years there has been a shift away from diagnostic angiography with the arrival on the market of high performance CT and MRI angiography systems which provide reliable and non-invasive alternatives.
Radiologists are by no means the only medical specialty performing interventional techniques as cardiologists and vascular surgeons have been quite successful in developing interventional skills, so much so that interventional cardiology has grown into a discipline of its own. In fields such as peripheral arterial disease treatment for example, it would seem that interventional radiologists have lost out to other specialties even though in some European countries like Germany they still have a significant share of this work. There is, however, a wide range of other areas, especially in interventional neuroradiology and oncology where interventional radiologists hold a quasi-monopoly.
In Europe, the Cardiovascular and Interventional Radiological Society of Europe (CIRSE) established in 2013 the first edition of the European Curriculum and Syllabus for Interventional Radiology which aimed at harmonizing training across European countries while supporting the European Board of Interventional Radiology (EBIR) examination in interventional radiology. CIRSE also works together with the European Society of Radiology (ESR) to attract more clinically-oriented medical students to interventional radiology. The steady growth of the ageing population in Europe and other industrialized countries and the resulting higher incidence of strokes and cancer cases combined with the multiplication and development of interventional techniques will boost the demand for interventional radiologists in the near future. Already now, there is a shortage of interventional radiologists in some countries, notably the UK where 25% of hospitals cannot provide minimally invasive procedures to their patients on a 24/7 basis because of a lack of recruitment of interventional radiologists in the National Health Service (NHS). This situation is having a clearly detrimental effect on patient care in some parts of the country. According to the Royal College of Radiologists (RCR), there are just 414 interventional radiologists in the NHS whereas 735 of them would be needed to provide 24/7 on-call service everywhere. In comparison, France has about 1,250 interventional radiologists while Germany totals over 1,000. In emerging countries, the shortages can be huge, such as in India where there are only 596 registered interventional radiologists, i.e. one per every 2,18 million population. The challenge for radiologists is to recognize the value of being close to the patient and embrace clinical care.


Despite significant inherent advantages of liquid chromatography-tandem mass spectrometry (LC-MS/MS) over immunoassay techniques in clinical laboratory applications, its adoption into routine practice has been slower than might have been expected. The barriers to more widespread uptake are a function of issues in the laboratory workflow. This article analyses those issues and discusses how they can be overcome by improved automation and integration with the laboratory information management system, drawing on examples from the North West London Pathology (NWLP) clinical laboratories at Imperial College Healthcare NHS Trust.
by Dr Emma L. Williams
Introduction
Liquid chromatography-tandem mass spectrometry (LC-MS/MS) has seen over two decades of use in specialist clinical laboratories in the UK, offering a number of significant advantages over immunoassay techniques. These advantages include increased specificity, sensitivity and accuracy, as well as the detection of multiple analytes within a single assay. There is no need for an antibody for analyte detection and the method is not susceptible to the antibody-based interferences that plague immunoassays [1]. LC-MS/MS is suitable for multiple sample matrices and avoids the need for radioactive tracers. LC-MS/MS assays also have a wider dynamic measurement range and have improved between-method bias when compared to immunoassays.
LC-MS/MS initially played a role in specialist clinical laboratories in areas such as newborn screening, inborn errors of metabolism, toxicology and in immunosuppressant and therapeutic drug monitoring. More recently LC-MS/MS has established a role in diagnostic endocrinology, with the first appearance of LC/MS-MS for the measurement of vitamin D in the international vitamin D external quality assurance scheme (DEQAS) in 2005. There are now over 150 labs registered in this scheme using LC/MS-MS for the measurement of vitamin D. However, automated immunoassay still dominates and represents 69% of participants registered in the DEQAS scheme. Why has there not been more widespread adoption?
A number of issues have inhibited wider adoption and routine use of LC/MS-MS in the clinical laboratory. First among these is the use of labour-intensive manual workflows, which result in lower throughput, decreased productivity and longer turnaround time. Furthermore, a high level of technical expertise is needed, not only for method development, but also for troubleshooting assay and equipment failures. In addition to the high initial capital costs of purchasing the equipment, ongoing personnel costs are higher because of the need for more technically competent staff. With a clear understanding of where the bottlenecks in the process arise, these barriers can be overcome.
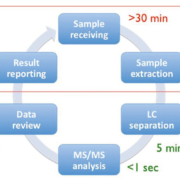
Figure 1 depicts the six main steps of a typical LC/MS-MS workflow, from sample receipt and extraction, separation in the LC, MS/MS analysis, data review and reporting of the results [2]. Of these steps it is the pre- and post-analytical stages that are the most time consuming and therefore if there is a focus on streamlining these, maximum benefit can be achieved. A number of steps can be taken to streamline the workflow, and these come under three broad headings of reduced manual processes, increased throughput and improved integration. Dependence on manual processes can be reduced by the automation of liquid handling and extraction, use of barcode reading for worklist generation and implementation of automated data analysis. Throughput can be increased with strategic column and sample management and by analyte multiplexing. Integration can be improved by bi-directional interfacing of the LC/MS-MS system to the laboratory information management system (LIMS) allowing automatic worklist upload and results download. These three strategic areas will be discussed in more detail below.
Reduced manual processes
Unlike the case with immunoassay, samples for LC-MS/MS usually require extraction prior to analysis. Historically this extraction step utilized liquid–liquid extraction or protein precipitation, these being carried out after the addition of internal standard to the calibrators, quality controls and patient samples. All of these steps involved manual pipetting and were very slow and time consuming. Use of an automated liquid-handling platform for the pipetting of samples and addition of internal standard allows some of the steps of liquid–liquid extraction and protein-precipitation methods to be automated. These liquid-handling platforms are available from a number of suppliers including Hamilton and Tecan.
With the advent of 96-well plate technology it became possible to carry out fully automated off-line solid phase extraction (SPE) using platforms such as the Freedom Evo (Tecan) and the Biomek NX (Beckman Coulter). More recently, supported liquid extraction (SLE), which allows solvent extraction to occur on a diatomaceous earth inert support, has also become available in a 96-well plate format. The Extrahera system (Biotage) enables automation of SLE by carrying out all of the pipetting and extraction steps required. In the NWLP laboratory, this system is used for the extraction of patient samples for vitamin D measurement by LC-MS/MS. A sample throughput of up to 50,000 samples per annum is achieved with capacity remaining for additional extractions for use in other LC-MS/MS applications. The system is robust and reliable with good pipetting precision and uses disposable pipette tips, thus avoiding sample carry over. Figure 2 depicts the Tecan Freedom Evo 200 and Biotage Extrahera liquid handlers in use in the NWLP laboratory.
In some manufacturers’ LC-MS/MS systems, on-line sample preparation and extraction is enabled by use of turbo flow or 2D chromatography. On-line protein precipitation and SPE is also now available using the Clinical Laboratory Automated sample preparation Module (CLAM)-2000 (Shimadzu Corporation) [3] and the Rapidfire 365 MS system (Agilent) [4] respectively. These latter examples most closely resemble the immunoassay workflow, whereby samples are introduced into the analytical system without any sample preparation or pre-treatment.
Increased throughput
Increased throughput can be achieved through the use of column and sample managers, allowing multiple assay batches to be queued up for overnight analysis of different LC-MS/MS assays. LC multiplexing enables multiple columns to be coupled to one tandem mass spectrometry system, maximizing the MS detection capability. In this approach, the use of quaternary solvent pumps in the LC enables column switching between different columns using different mobile phases. Finally there is analyte multiplexing, which can use manufacturers’ kits or in-house laboratory developed tests (LDTs). This approach enables multiple analytes to be detected in a single chromatographic separation by the use of multiple reaction monitoring for MS/MS detection. Perkin Elmer and Chromsystems both provide kits enabling the simultaneous measurement of multiple steroid hormones within a single assay panel. In the NWLP laboratory an in-house LDT steroid panel for the simultaneous measurement of androstenedione, 17-hydroxyprogesterone and testosterone has been implemented. This multiplexed assay has replaced the previous stand-alone assays for these analytes, thus increasing throughput and offering faster turnaround time. The assay utilizes off-line SPE using Waters Oasis PRiME HLB 96-well plates and the Tecan Freedom Evo 200 automated liquid handler [5].
Improved integration
Improved integration can be achieved by the use of bi-directional interfacing between the LIMS and the LC-MS/MS instrument software. Nowadays, manufacturers of LC-MS/MS systems offer customer support to allow their systems to be interfaced to the LIMS. One example is the MassLynx LIMS interface (Waters), which enables both worklist download and results upload. The MassLynx LIMS interface is accessed via the LC-MS/MS system software allowing sample worklists, created by barcode scanning of the patient samples, to be imported directly. Following peak integration and analyte quantitation the results are directly transmitted from the LC-MS/MS to the LIMS via an HL7 interface. This avoids the need for manual transcription thus saving a great deal of staff time and eliminating transcription errors.
The ultimate aim of LC-MS/MS integration is to achieve complete integration of LC-MS/MS instruments into the automated workflow of high-throughput routine clinical laboratories. With the recent launch of the Cascadion LC-MS/MS analyser (Thermo Fisher Scientific) this ultimate aim has now been achieved [6]. This analyser offers a complete LC-MS/MS solution including primary blood tube sampling, on-board sample extraction, LIMS connectivity and a random access workflow enabling the provision of a 24/7 service. Traceable manufacturer’s kits are offered for the measurement of a panel of immunosuppressant drugs, testosterone and vitamin D with further assay kits in the development pipeline. The Cascadion analyser is shown in Figure 3.
Summary
LC/MS-MS automation and integration is now a reality, allowing faster sample processing and improved turnaround time, as well as offering increased staff productivity, improved quality and reduced error rate. Staff time is liberated for further service development, allowing the more rapid introduction of validated in-house LDTs into the assay repertoire. Finally there is the possibility of complete analyser integration allowing routine, high-throughput analysis, as is already the standard approach for the common immunoassay platforms. This exciting development will support the more widespread adoption of LC-MS/MS in the routine clinical laboratory by offering complete automation and integration, overcoming the barriers discussed in this article and enabling the inherent advantages of LC/MS-MS in clinical laboratory practice to be more fully realized.
References
1. Jones AM, Honour JW. Unusual results from immunoassays and the role of the clinical endocrinologist. Clin Endocrinol Oxf 2006; 64: 234–244.
2. Zhang YV, Rockwood A. Impact of automation on mass spectrometry. Clin Chim Acta 2015; 450: 298–303.
3. Shimadzu. CLAM-2000. Fully automated sample preparation module for LCMS. (https://www.shimadzu.com/an/lcms/clam/index.html).
4. Jannetto PJ, Langman LJ. High-throughput online solid-phase extraction tandem mass spectrometry: Is it right for your clinical laboratory? Clin Biochem 2016; 49: 1032–1034.
5. Williams EL. LC-MS/MS measurement of serum steroids in the clinical laboratory. Clinical Laboratory International 2017; Sept: 18–20.
6. ThermoFisher Scientific. Cascadion SM Clinical Analyzer (www.thermofisher.com/cascadion).
The author
Emma L. Williams PhD, FRCPath
North West London Pathology, Imperial College Healthcare NHS Trust, London, UK
E-mail: emma.walker15@nhs.net

Danish, Finnish and Swedish organizations join forces to facilitate business partnering and networking at Arab Health 2018. At the event, 75 Nordic companies bring innovative life science solutions aiming to add sustainable value to the Middle East healthcare sectors and to build lasting relations between the Nordic participants and local stakeholders.
Business Finland, Business Sweden, Danish Health Tech Group and Global Pharma Consulting are coordinating four national pavilions at Arab Health 2018. To kick off the trade fair, the organizations announce an exclusive Nordic Business Partnering and Networking Reception for invited guests on Monday 29 January 2018 at 7-10 pm at the Sofitel Dubai Downtown.
“This is the only opportunity for stakeholders in the MENA region to talk to so many decision makers, officials and experts from the Nordics in one place in a relaxed setting,” explains Senior Consultant Paula Hassoon at Global Pharma Consulting, organizer of The Innovation Pavilion by Sweden.
“Joining forces with our Danish and Finnish colleagues to host a Nordic partnering and networking event brings added value to all of the participating companies,” she says.
Digital health from Finland
At the four national pavilions, the Nordic companies will showcase cutting-edge med-tech solutions and technologies to the MENA region. According to Meria Heikelä, Director at Business Finland and co-organiser of the Finnish pavilion, Finland ranks among the three strongest health technology economies in the world, with digital health being its largest high-tech export.
“Finland’s world-class research and technology competencies are the pinnacle of its health sector and one reason why Finland has one of the most efficient healthcare systems in the world. Preventive healthcare and rehabilitation solutions are among the key focus areas of Finland at Arab Health 2018,” explains Meria Heikelä.
Danish innovations in med-tech
With the annual Pavilion of Denmark at Arab Health and a recent business delegation visit to UAE and Saudi Arabia healthcare sectors, Danish Health Tech Group is committed to share the Danish med-tech strengths with stakeholders in the MENA region.
“In Denmark, we prioritize design and quality, and innovate through an inherent focus on public-private sector cooperation and by proactively involving patients and staff in the healthcare sector,” says Thomas Andersen, Head of Danish Health Tech Group.
Swedish world-class healthcare
While all the Danish companies are exhibiting with Danish Health Tech Group, Sweden offers two different pavilions.
The Innovation Pavilion by Sweden and the official Swedish pavilion each has representatives from 20 Swedish healthcare and life science companies.
“Sweden is known for its world-class’ innovations within the healthcare sector. Much of this success derives from the tradition of entrepreneurship through the close collaboration between the government, academia and industry,” says Fredrik Bodin, Trade Commissioner of Sweden to the UAE, co-organizer of the official Swedish pavilion.
The national pavilions at Arab Health 2018
More information to be obtained from:
Business Finland (Finpro) at www.finpro.fiBusiness Sweden’s at www.business-sweden.seDanish Health Tech Group at www.dk-healthtech.comGlobal Pharma Consulting at www.globalpharma.se

Earlier this year the American Medical Association (AMA) published an article entitled ‘Lower costs by going green!’ aimed at the healthcare sector. They note that, in the USA, 9 – 10 percent of the nation’s total carbon dioxide emissions are generated by the health care industry – and the USA is not alone in this high carbon footprint. In Europe the average emissions is estimated to be about 5 percent. Cleary there is a margin for improvement. The AMA article makes practical, money and energy saving proposals aimed at the small medical practices. The question arises as to how this could be achieved in the larger hospital environment. There is a trove of excellent suggestions for building new energy efficient and environmentally friendly hospitals – but what of existing hospitals?
A very useful source of information is the Global Green and Healthy Hospitals (GGHH) community. The community of almost 1000 members have the aim to transform the health sector and foster a healthy future for people and the planet. To achieve this aim GGHH brings together hospitals, health systems, and health organizations from around the world under the shared goal of reducing the environmental footprint of the health sector.
To achieve their aims, they suggest a 10 goal strategy: Leadership -making environmental health, safety and sustainability key organizational priorities; substituting harmful chemicals with safer alternatives; to reduce, treat and safely dispose of healthcare waste; to reduce water consumption, as well as to source, purchase and serve sustainably locally grown, healthy food. Other goals include implementing energy saving strategies; safely manage and dispose of pharmaceuticals; transportation planning, building efficiency design; and purchasing safe and sustainable products.
GGHH points out that there is not one model of green and healthy hospital but indicate that many health systems around the world are already taking steps to reduce their environmental footprint contributing to public health while at the same time saving money. Initiatives such as the ‘Health Promoting Hospital Network’ originating in Europe and with the support of the World Health Organisation, is developing a set of sustainability criteria. Such initiatives and conferences of greening the health sector are emerging in countries as diverse as Argentina, China, India, South Africa and Sweden – to name a few.
The Global Green and Healthy Hospitals agenda sets out to support these existing efforts around the world to promote greater sustainability and environmental health. European hospitals would do well to align themselves with this community, reducing the European healthcare contribution to the carbon footprint, as well as, in many cases, saving money –immediately and in the future.
The Health Industry Summit (tHIS) 2017 hosted by China and organized by Reed Sinopharm, was held in Shanghai at the National Exhibition and Convention Center from May 15th to 18th with well over 200,000 healthcare industry professionals from more than 150 countries and regions in attendance.
Now in its third edition, tHIS has been firmly established as the world’s largest health industry event with over 350,000 square meters of exhibition space and 160 individual events and conferences. It comes at a crucial time as China drives forward its “Healthy China 2030 Plan” initiative to realize among other goals an industry growth target of RMB 16 trillion (USD 2.3 trillion, Euro 1.9 trillion) by 2030 and an increase of average citizen lifespan by 3 years to 79 years.
Key events at tHIS 2017 included China’s three top medical equipment and pharmaceutical exhibitions (CMEF, PHARMCHINA and API China) and the leading healthcare investment forum – Healthcare China 2017. This year’s investment forum was co-organized by Reed Sinopharm, JP Morgan Asset management, CICC and Sinopharm Capital and was attended by more than 1000 CEOs, investors and institutions.
The exhibition featured the entire industry value chain and showcased tens of thousands of the latest technologies and products. Emerging technologies such as VR, AR, wearables and AI featured strongly on the show floor as well as in the key forums. During tHIS 2017, the World Medical Robots Innovation and Development Summit was held to reflect the growing trend for robotics and AI applications.
Over 7000 exhibiting companies from 30 countries were at the show including medical device giants like GE, United Imaging, Siemens, Philips and Mindray as well as major pharmaceutical groups in China including Sinopharm, Shanghai Pharma and CR Pharmaceuticals. The majority of the most innovative companies in the medical field choose CMEF as their global or Asia Pacific new product launch platform and more than 600 new product launches took place during the 4 days of the show. Among the new products released, United imaging launched its uVR 4D vision explorer platform, enabling more detailed dissect structure and spatial information, while GE launched its first cloud-based digital application for medical equipment management APM (asset performance management), which was developed by their China team. BGI also attended with their gene sequencer BGISEQ-500, a benchtop high-throughput open sequencing platform that provides end-to-end solutions.
Natural Health and Nutrition Expo were among the fastest growing segments in the portfolio, helped by the expected population boom in light of the reversal of the single child policy last year as well as a growing health-conscious middle class in China. Popular international brands like Blackmores, Nature Made and Garden of Life made their debut at the show along with 700 suppliers of health food and supplements, bringing with them popular product lines tailored to the Chinese market.
The Health Industry Summit is organized by Reed Sinopharm, a joint venture between the world’s leading event organizer Reed Exhibitions and China’s leading state-owned medical & pharmaceutical group Sinopharm, ranked number 199 on the latest Fortune 500 list released in July. Its next edition will be held in April 2018 in Shanghai while the 78th China International Medical Equipment Fair (CMEF Autumn 2017) is to take place in Yunnan at the Kunming Dianchi Convention & Exhibition Centre from October 29 to November 1.
Visitor profile
The vast majority of visitors naturally came from China, covering all regions and healthcare sectors. However, there was also a growing segment of international visitors. Topping the list of foreign countries was India with a 20% share of international attendees followed by Korea (15%), Pakistan, Japan, USA, Russia and Germany.
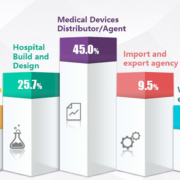
Overall, CMEF visitors spanned the entire medical area – both healthcare and medical device industry. Distributors of medical devices constituted the largest single visitor group with 45% of the total followed by hospital build and design (26%) and rehabilitation centre professionals (see detailed visitor composition chart on previous page).
National pavilions
The international participation is increasing, reflecting the growing importance of China’s healthcare industry. Further adding to the show’s attraction, a large number of national pavilions were featured in a dedicated hall where a constant stream of visitors could view the latest products and technology of companies from countries as diverse as Switzerland, Canada, Taiwan or Germany. For the first time the US and Pakistan had country group exhibits while the Spanish Medical Technology Association (FENIN) led some Spanish companies to make their appearance at the CMEF Spanish pavilion and the German Land of Thuringia organized a regional exhibit for the first time.
Prins Hendrikstraat 1
5611HH Eindhoven
The Netherlands
info@interhospi.com
PanGlobal Media IS not responsible for any error or omission that might occur in the electronic display of product or company data.
