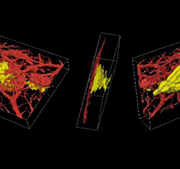
Acoustic angiography – towards new tumour morphology metrics
Acoustic angiography is a method to acquire images that possess both high resolution as well as a superior contrast-to-tissue ratio. As opposed to clinical

Acoustic angiography is a method to acquire images that possess both high resolution as well as a superior contrast-to-tissue ratio. As opposed to clinical

From 5 to 8 March 2015, the 31st Korea International Medical & Hospital Show in Seoul brought together domestic and overseas manufacturers and medical professionals.
More than 72,000 visitors convened last March to the COEX exhibition centre where KIMES is taking place every year. The 2015 edition saw 1145 companies showcasing their products over 38,350 square meters of exhibition space. Among exhibitors, the highest number unsurprisingly was from Korea, represented by 530 manufacturers, followed by China (137), the US (117), Germany (96) and Japan (67).
According to the post-show survey carried out by the organizers, a majority of exhibitors obtained positive results and fruitful contacts with qualified visitors at KIMES 2015. Most of them also reported that the medical market was continuing to grow in the Asia region. This is one of the main factors driving the expansion of Korea



The costly critical care provided by highly qualified personnel using state-of-the-art equipment in today

The Internet of Things (IoT) has been hailed by some commentators as one of the biggest revolutions in the hospital environment since the inception of patient monitoring equipment thirty years ago.
The latter triggered dramatic improvements in outcomes and explains the panoply of equipment now standard in every hospital room – from pulse oximeters, ECGs and apnea monitors to infusion pumps and ventilators.
False positives and negatives
Few doubt that healthcare today has improved because of such equipment. However, as the devices proliferated, another kind of risk has emerged. These monitoring devices operate independently, with no means to assimilate information from multiple sources and intelligently understand patient status. As a result, some devices can occasionally fail to issue an alarm (a false negative), while others do so wrongly (a false positive). On their part, healthcare staff members – whose numbers have shrunk as many of their tasks began to be handled by the devices – often tend to shut off what they believe are nuisance alarms.
Many are just that – nuisances. Some are not. In both cases of false positives and false negatives, human lives are often put at risk.
Nine of 10 healthcare IT departments ready for IoT
The Internet of Things (IoT) is seen to offer a way out of such challenges. IoT uses sensors, radio-frequency identification (RFID) and Real Time Location System (RTLS) to capture or monitor data and automatically trigger certain events.
In times past, healthcare sensors covered devices such as vital signs monitors. Today, those monitors and much other hospital equipment is connected by the IoT

A wave of new anesthetic agents on the market has been followed by intense interest in the cost-effectiveness of different anesthesia alternatives. This, however, is not something new.
Debate dates back 50 years
Attention to the economics of anesthesia use dates back a half century. In 1965, the
Prins Hendrikstraat 1
5611HH Eindhoven
The Netherlands
info@interhospi.com
PanGlobal Media IS not responsible for any error or omission that might occur in the electronic display of product or company data.
