A prostate cancer detection software system to help pathologists quickly identify suspicious areas of tissue, developed by Paige, will be investigated in a multicentre clinical study led by Oxford University as part of a successful NHSx Artificial Intelligence Health and Care Award application.
Paige Prostate automatically detects and highlights areas of suspicious tissue, allowing the pathologist to quickly identify if cancer is present in the patient biopsy. The software also measures and grades the severity of tumours it detects, all of which assists the pathologist in accurately and efficiently diagnosing cancer and influencing important treatment decisions in patients with prostate cancer.
This award means that Oxford University and its NHS partners North Bristol NHS Trust and University Hospitals Coventry and Warwickshire, together with Oxford University Hospitals NHS Foundation Trust, will use Paige Prostate prospectively in a real-world cancer laboratory setting, taking the technology one step closer to widespread use in the NHS to benefit patients.
AI Award
Oxford University was one of five lead organisations to receive Phase 4 funding, which was announced by the Health and Social Care Secretary Matt Hancock on 16 June 2021. The AI Award is a significant government initiative making £140 million available over four years to accelerate the testing and evaluation of artificial intelligence technologies which meet the aims set out in the NHS Long Term Plan.
Professor Clare Verrill from Oxford University’s Nuffield Department of Surgical Sciences and Oxford University Hospitals NHS Foundation Trust and Principle Investigator on the project, said, ‘I see this both as a natural evolution and key transformational point for histopathology. With this award we can advance the adoption of powerful technology to help pathologists by demonstrating the system-wide potential of using AI-based diagnostic systems in routine reporting.’
Dr Margaret Horton, Business Lead for Europe at Paige and a co-Investigator on the project said: “The NHSx program provides the ideal catalyst for the system-wide adoption of artificial intelligence-based technologies such as Paige Prostate to improve efficiency, accuracy and patient and staff experiences. The pathologists and principal investigators in this study are global leaders in the implementation of digital pathology and utilising innovation to advance diagnostic service delivery.”
Dr Leo Grady, Chief Executive Officer of Paige, commented: “Computational pathology for diagnostics has clear potential to increase diagnostic accuracy and more efficiently utilise scarce diagnostic resources in the NHS and in other health systems around the world. The next clear step to bring this to routine practice is pathologist-led implementation in every day practice to demonstrate and measure benefits to patients, laboratories and the NHS. This exciting work with Oxford University and their NHS partners is a tremendous achievement and Paige is very proud to be working with them in transforming the important work that pathologists do.”
The AI Award is one of the programmes that make up the NHS AI Lab, led by NHSX and delivered in partnership with the Accelerated Access Collaborative (AAC) and National Institute for Health Research (NIHR).
Dr Indra Joshi, Director of AI, NHSX, said: “With this latest round of AI Award winners, we now have an incredible breadth of expertise across a wide range of clinical and operational areas. Through this award, Oxford University and its NHS partners will be at the forefront of applying artificial intelligence in new ways to transform health and care.”
https://interhospi.com/wp-content/uploads/sites/3/2021/07/paige_prostate_pathology.jpg840980panglobalhttps://interhospi.com/wp-content/uploads/sites/3/2020/06/Component-6-–-1.pngpanglobal2021-07-15 09:49:422021-07-15 09:49:42Oxford University, partners to evaluate Paige Prostate Cancer Detection System
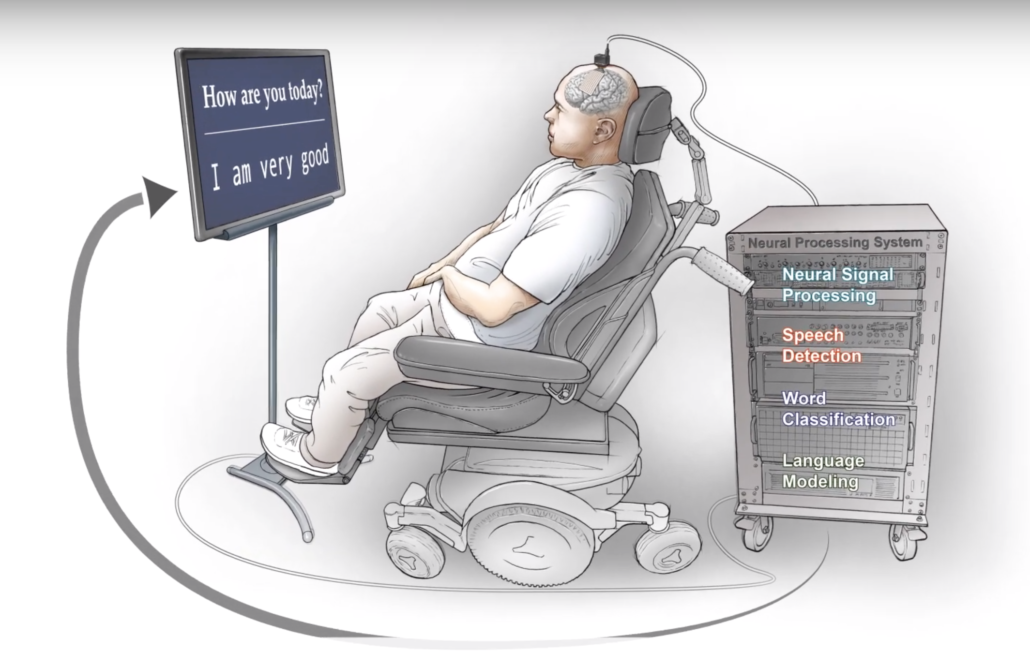
Researchers at UC San Francisco have successfully developed a ‘speech neuroprosthesis’ that has enabled a man with severe paralysis to communicate in sentences, translating signals from his brain to the vocal tract directly into words that appear as text on a screen.
The achievement, which was developed in collaboration with the first participant of a clinical research trial, builds on more than a decade of effort by UCSF neurosurgeon Edward Chang, MD, to develop a technology that allows people with paralysis to communicate even if they are unable to speak on their own. The study appears July 15 in the New England Journal of Medicine.
“To our knowledge, this is the first successful demonstration of direct decoding of full words from the brain activity of someone who is paralyzed and cannot speak,” said Chang, the Joan and Sanford Weill Chair of Neurological Surgery at UCSF, Jeanne Robertson Distinguished Professor, and senior author on the study. “It shows strong promise to restore communication by tapping into the brain’s natural speech machinery.”
Each year, thousands of people lose the ability to speak due to stroke, accident, or disease. With further development, the approach described in this study could one day enable these people to fully communicate.
Previously, work in the field of communication neuroprosthetics has focused on restoring communication through spelling-based approaches to type out letters one-by-one in text. Chang’s study differs from these efforts in a critical way: his team is translating signals intended to control muscles of the vocal system for speaking words, rather than signals to move the arm or hand to enable typing. Chang said this approach taps into the natural and fluid aspects of speech and promises more rapid and organic communication.
“With speech, we normally communicate information at a very high rate, up to 150 or 200 words per minute,” he said, noting that spelling-based approaches using typing, writing, and controlling a cursor are considerably slower and more laborious. “Going straight to words, as we’re doing here, has great advantages because it’s closer to how we normally speak.”
Over the past decade, Chang’s progress toward this goal was facilitated by patients at the UCSF Epilepsy Center who were undergoing neurosurgery to pinpoint the origins of their seizures using electrode arrays placed on the surface of their brains. These patients, all of whom had normal speech, volunteered to have their brain recordings analyzed for speech-related activity. Early success with these patient volunteers paved the way for the current trial in people with paralysis.
Previously, Chang and colleagues in the UCSF Weill Institute for Neurosciences mapped the cortical activity patterns associated with vocal tract movements that produce each consonant and vowel. To translate those findings into speech recognition of full words, David Moses, PhD, a postdoctoral engineer in the Chang lab and one of the lead authors of the new study, developed new methods for real-time decoding of those patterns and statistical language models to improve accuracy.
But their success in decoding speech in participants who were able to speak didn’t guarantee that the technology would work in a person whose vocal tract is paralyzed. “Our models needed to learn the mapping between complex brain activity patterns and intended speech,” said Moses. “That poses a major challenge when the participant can’t speak.”
In addition, the team didn’t know whether brain signals controlling the vocal tract would still be intact for people who haven’t been able to move their vocal muscles for many years. “The best way to find out whether this could work was to try it,” said Moses.
BRAVO1 speaks
To investigate the potential of this technology in patients with paralysis, Chang partnered with colleague Karunesh Ganguly, MD, PhD, an associate professor of neurology, to launch a study known as “BRAVO” (Brain-Computer Interface Restoration of Arm and Voice). The first participant in the trial is a man in his late 30s who suffered a devastating brainstem stroke more than 15 years ago that severely damaged the connection between his brain and his vocal tract and limbs. Since his injury, he has had extremely limited head, neck, and limb movements, and communicates by using a pointer attached to a baseball cap to poke letters on a screen.
The participant, who asked to be referred to as BRAVO1, worked with the researchers to create a 50-word vocabulary that Chang’s team could recognize from brain activity using advanced computer algorithms. The vocabulary – which includes words such as “water,” “family,” and “good” – was sufficient to create hundreds of sentences expressing concepts applicable to BRAVO1’s daily life.
For the study, Chang surgically implanted a high-density electrode array over BRAVO1’s speech motor cortex. After the participant’s full recovery, his team recorded 22 hours of neural activity in this brain region over 48 sessions and several months. In each session, BRAVO1 attempted to say each of the 50 vocabulary words many times while the electrodes recorded brain signals from his speech cortex.
From neural activity to words
To translate the patterns of recorded neural activity into specific intended words, the other two lead authors of the study, Sean Metzger, MS and Jessie Liu, BS, both bioengineering doctoral students in the Chang Lab used custom neural network models, which are forms of artificial intelligence. When the participant attempted to speak, these networks distinguished subtle patterns in brain activity to detect speech attempts and identify which words he was trying to say.
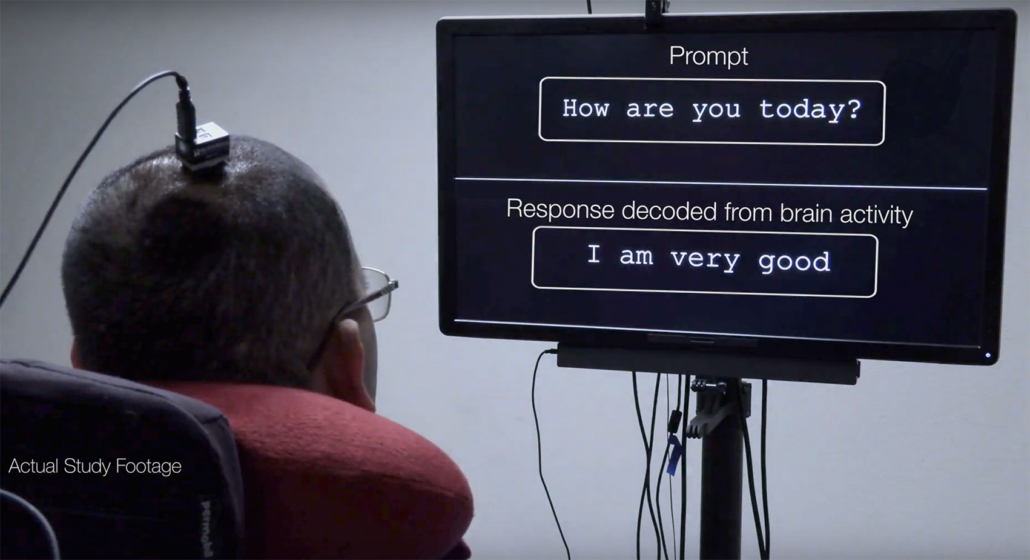
To test their approach, the team first presented BRAVO1 with short sentences constructed from the 50 vocabulary words and asked him to try saying them several times. As he made his attempts, the words were decoded from his brain activity, one by one, on a screen.
Then the team switched to prompting him with questions such as “How are you today?” and “Would you like some water?” As before, BRAVO1’s attempted speech appeared on the screen. “I am very good,” and “No, I am not thirsty.”
The team found that the system was able to decode words from brain activity at rate of up to 18 words per minute with up to 93 percent accuracy (75 percent median). Contributing to the success was a language model Moses applied that implemented an “auto-correct” function, similar to what is used by consumer texting and speech recognition software.
Moses characterized the early trial results as a proof of principle. “We were thrilled to see the accurate decoding of a variety of meaningful sentences,” he said. “We’ve shown that it is actually possible to facilitate communication in this way and that it has potential for use in conversational settings.”
Looking forward, Chang and Moses said they will expand the trial to include more participants affected by severe paralysis and communication deficits. The team is currently working to increase the number of words in the available vocabulary, as well as improve the rate of speech.
Both said that while the study focused on a single participant and a limited vocabulary, those limitations don’t diminish the accomplishment. “This is an important technological milestone for a person who cannot communicate naturally,” said Moses, “and it demonstrates the potential for this approach to give a voice to people with severe paralysis and speech loss.”
Research co-authors
Co-authors on the paper include Sean L. Metzger, MS; Jessie R. Liu; Gopala K. Anumanchipalli, PhD; Joseph G. Makin, PhD; Pengfei F. Sun, PhD; Josh Chartier, PhD; Maximilian E. Dougherty; Patricia M. Liu, MA; Gary M. Abrams, MD; and Adelyn Tu-Chan, DO, all of UCSF. Funding sources included National Institutes of Health (U01 NS098971-01), philanthropy, and a sponsored research agreement with Facebook Reality Labs (FRL), which completed in early 2021.
Reference
Neuroprosthesis for Decoding Speech in a Paralyzed Person with Anarthria. New England Journal of Medicine, 2021; 385 (3): 217 DOI: 10.1056/NEJMoa2027540
https://interhospi.com/wp-content/uploads/sites/3/2021/07/neuro_1_web.jpg9271417panglobalhttps://interhospi.com/wp-content/uploads/sites/3/2020/06/Component-6-–-1.pngpanglobal2021-07-15 09:01:132021-07-15 09:01:13BREAKTHROUGH: researchers develop neuroprosthesis that enables paralyzed man to communicate with words
By Tracy Hussell Professor of Inflammatory Disease, University of Manchester
Late last year, I asked: is it safe to have more than one type of COVID-19 vaccine? A trial has now addressed that question, as well as what effect combining different vaccine types has on immunity.
Most COVID-19 vaccines require two doses, and the usual strategy is to give people the same vaccine type for both. But the Com-Cov study, led by the University of Oxford, recruited over 800 participants from across the UK to investigate the effects of giving people different vaccines for their first and second jabs. Two vaccines were studied: those made by Pfizer and AstraZeneca.
So, is mix and match an option? The trial’s results are preliminary, having yet to be reviewed by other scientists, but the answer appears to be yes. Giving people different types of COVID-19 vaccine appears not only to be safe, but also a potential way of boosting protection against the coronavirus.
However, the exact benefits depend on which vaccine goes first and which second. Taking the AstraZeneca vaccine followed by the Pfizer one resulted in a striking increase in antibodies against the coronavirus’s spike protein (a key part of its outer structure) compared to using the AstraZeneca vaccine for both doses or Pfizer followed by AstraZeneca.
Taking the AstraZeneca vaccine followed by Pfizer resulted in a better T cell response than all other combinations of doses. T cells – also known as T lymphocytes – are immune cells that help kill invading germs (such as the coronavirus) and support antibody production.
The Com-Cov study will next look at whether mixing and matching doses like this provides as good results when a larger gap is left between doses. The time between doses in this initial trial was 28 days, but a parallel study is stretching this to 84 days. The results are yet to be reported.
An expected outcome?
Other researchers have also been studying mixing vaccine types to fight COVID-19. A Spanish study recently reported that people who initially received the AstraZeneca vaccine experienced a massive increase to their antiviral immunity when given a second dose of the Pfizer vaccine – providing more evidence that Pfizer works well as a booster.
To understand why these beneficial effects might be happening, it’s important to understand how the AstraZeneca and Pfizer vaccines work. Both present a key element of the coronavirus – again, the spike protein – to the immune system, but do so using different methods.
The Pfizer approach packs the genetic code for the coronavirus’s spike protein into fatty nanoparticles. When these particles enter the body’s cells, the code is read and copies of the spike protein are produced, leading to an immune response. The AstraZeneca vaccine delivers the same genetic code but uses a weakened form of a common cold virus (an adenovirus) from chimpanzees to carry the code into cells.
When the first vaccine doses are given, it is possible that an immune response is raised not just against the spike protein created, but also against the carriers that are used to deliver the code for it. This is a known issue for treatments or vaccines that use viruses for delivery. If the second dose is then the same, the immunity developed against the carrier will react against the second dose, clearing some of it before robust, protective and long-lasting immunity develops.
This is why Russia’s Sputnik V vaccine – which is based on the same delivery method as the AstraZeneca vaccine – uses two different adenoviruses as carriers for its first and second doses, and has achieved impressive results.
Why mixing doses is so important
There are additional benefits to mixing vaccine doses on top of improving protection. Logistical problems can arise when a second vaccine dose has to be identical to the first. Producing double the quantity of one vaccine takes time. Boosting with a different vaccine could allow the world’s population to be vaccinated quicker.
Second, if a person reacts badly to their first vaccination, they are more likely to get a second dose if they know it is a different one – and it’s clear that two are needed for good protection. Governments may also decide a certain type of vaccine is less suitable for different groups of people, as has been the case with the AstraZeneca vaccine in younger people in some countries. Having more potential vaccine combinations available may help overcome any public uncertainty in the wake of these sorts of decisions.
Supplying vaccines to some low- and middle-income countries can also be difficult, particularly if they do not have the necessary cold storage requirements for large batches of a vaccine that need to be kept at low temperatures. Including vaccines into the distribution plan that do not need storage at very low temperatures may make widespread vaccine delivery easier.
So there are clearly huge benefits to vaccine mixing. However, this study only looked at two vaccine types – in time, every combination will need to be tested, in every age group and in every ethnicity. Vaccines may also behave differently if mixed in different contexts, for example, against a backdrop of malnutrition or other infectious diseases. These factors will need to be included in future testing too. But for now, this study suggests that a mix-and-match approach to COVID-19 vaccines is an acceptable, useful option.
This article was originally published in The Conversation. It is republished here under a Creative Commons licence.
https://interhospi.com/wp-content/uploads/sites/3/2021/07/covid_vaccine.jpg12721920panglobalhttps://interhospi.com/wp-content/uploads/sites/3/2020/06/Component-6-–-1.pngpanglobal2021-07-06 08:11:062021-07-06 08:11:06COVID vaccines: combining AstraZeneca and Pfizer may boost immunity – new study
The International Hospital Federation (IHF) recognizes that many hospitals and healthcare organizations around the globe are still caught up in the fight against COVID-19 and decided to extend the deadline and provide more time for everyone to prepare their entries for the IHF awards.
“The COVID-19 pandemic continues to create havoc globally and has put our healthcare providers and systems under unimaginable strain. However, in response to this pandemic, we are delighted to see that hospitals and healthcare organizations around the world also produced outstanding and innovative projects to combat COVID-19 worthy of worldwide recognition. We would like this year’s IHF Awards to be dedicated as a platform for these projects to be highlighted and serve as inspiration to others,” Ronald Lavater, CEO of the International Hospital Federation said.
The process for submitting entries is straightforward. The IHF has awards in the following categories:
Dr. Kwang Tae Kim Grand Hospital Award
Austco Excellence Award for Quality and Patient Safety
American College of Healthcare Executives Excellence Award for Leadership and Management
Ashikaga – Nikken Excellence Award for Green Hospitals
Sultanate of Oman Excellence Award for Health Services During Crisis
Excellence Award for Corporate Social Responsibility
The awards will be presented during a special ceremony at the 44th IHF World Hospital Congress which will be held from 8-11 November 2021 in Barcelona, Spain.
If you have questions or need assistance with your entries, email: awards@ihf-fih.org.
https://interhospi.com/wp-content/uploads/sites/3/2021/07/IHF-barcelona.jpg454454panglobalhttps://interhospi.com/wp-content/uploads/sites/3/2020/06/Component-6-–-1.pngpanglobal2021-07-01 14:13:162021-07-01 14:13:16Submission of entries for IHF Awards extended to 31 July
We may ask you to place cookies on your device. We use cookies to let us know when you visit our websites, how you interact with us, to enrich your user experience and to customise your relationship with our website.
Click on the different sections for more information. You can also change some of your preferences. Please note that blocking some types of cookies may affect your experience on our websites and the services we can provide.
Essential Website Cookies
These cookies are strictly necessary to provide you with services available through our website and to use some of its features.
Because these cookies are strictly necessary to provide the website, refusing them will affect the functioning of our site. You can always block or delete cookies by changing your browser settings and block all cookies on this website forcibly. But this will always ask you to accept/refuse cookies when you visit our site again.
We fully respect if you want to refuse cookies, but to avoid asking you each time again to kindly allow us to store a cookie for that purpose. You are always free to unsubscribe or other cookies to get a better experience. If you refuse cookies, we will delete all cookies set in our domain.
We provide you with a list of cookies stored on your computer in our domain, so that you can check what we have stored. For security reasons, we cannot display or modify cookies from other domains. You can check these in your browser's security settings.
.
Google Analytics Cookies
These cookies collect information that is used in aggregate form to help us understand how our website is used or how effective our marketing campaigns are, or to help us customise our website and application for you to improve your experience.
If you do not want us to track your visit to our site, you can disable this in your browser here:
.
Other external services
We also use various external services such as Google Webfonts, Google Maps and external video providers. Since these providers may collect personal data such as your IP address, you can block them here. Please note that this may significantly reduce the functionality and appearance of our site. Changes will only be effective once you reload the page
Google Webfont Settings:
Google Maps Settings:
Google reCaptcha settings:
Vimeo and Youtube videos embedding:
.
Privacy Beleid
U kunt meer lezen over onze cookies en privacy-instellingen op onze Privacybeleid-pagina.