


Respiratory tract infection (RTI) is the fourth leading cause of mortality globally resulting in around three million deaths per annum, predominantly from pneumonia. In the West, whilst RTIs do not wreak the same toll that they do in the lower income countries, they are the most frequent reason for consulting a general practitioner (GP). The majority of RTIs affect the upper respiratory tract and are of viral origin; numerous studies conclude that there is no benefit in prescribing antimicrobials for an acute uncomplicated RTI. And as currently one of the most serious global healthcare concerns is antimicrobial resistance (AMR), it is imperative that diagnosis and treatment at primary care level do not augment this problem. Relevant national guidelines exist in most European countries, but there are considerable variations across the EU in the frequency that antimicrobials are prescribed for patients with RTIs, ranging from 28% in the Netherlands to 92% in Greece.
Point-of-care testing by GPs, however, can allow more prudent use of antimicrobials. GPs are being encouraged to measure C reactive protein (CRP), a very early marker of inflammation produced by the liver, as an adjunct to clinical examination. Serum levels increase within six hours of infection, peak within two to three days and decline rapidly to baseline level once the infection is resolved. Bacterial infections result in high levels >100 mg/L, whereas levels in viral infections rarely exceed 50 mg/L. And a cost-effective CRP POC test that can be performed within five minutes is available. Although serum procalcitonin level is more specific for distinguishing between bacterial and viral infections, the POC tests for this analyte currently take longer to obtain a result and are thus more suitable for hospital settings. The consensus from European consortia concerned with managing RTI patients and combating antimicrobial resistance is that patients with CRP levels <20 mg/L should not be prescribed antimicrobials, those with levels >100 mg/L should, and for those with levels in between signs, symptoms and risk factors should all be scrutinized and antimicrobials prescribed if symptoms worsen. This approach appears to be acceptable to both patients and GPs.
Randomized clinical trials have been carried out in several countries comparing

The Internet of Things (IoT) has been hailed by some commentators as one of the biggest revolutions in the hospital environment since the inception of patient monitoring equipment thirty years ago.
The latter triggered dramatic improvements in outcomes and explains the panoply of equipment now standard in every hospital room – from pulse oximeters, ECGs and apnea monitors to infusion pumps and ventilators.
False positives and negatives
Few doubt that healthcare today has improved because of such equipment. However, as the devices proliferated, another kind of risk has emerged. These monitoring devices operate independently, with no means to assimilate information from multiple sources and intelligently understand patient status. As a result, some devices can occasionally fail to issue an alarm (a false negative), while others do so wrongly (a false positive). On their part, healthcare staff members – whose numbers have shrunk as many of their tasks began to be handled by the devices – often tend to shut off what they believe are nuisance alarms.
Many are just that – nuisances. Some are not. In both cases of false positives and false negatives, human lives are often put at risk.
Nine of 10 healthcare IT departments ready for IoT
The Internet of Things (IoT) is seen to offer a way out of such challenges. IoT uses sensors, radio-frequency identification (RFID) and Real Time Location System (RTLS) to capture or monitor data and automatically trigger certain events.
In times past, healthcare sensors covered devices such as vital signs monitors. Today, those monitors and much other hospital equipment is connected by the IoT
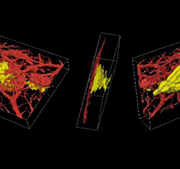
Acoustic angiography is a method to acquire images that possess both high resolution as well as a superior contrast-to-tissue ratio. As opposed to clinical
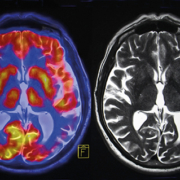
PET/MRI is a hybrid combination of two imaging modalities. The first consists of positron emission tomography (PET) for ultra-sensitive imaging of metabolism and tracking uniquely labelled cell types or cell receptors. The second consists of the structural and functional characterization of tissue provided by magnetic resonance imaging (MRI).
The combination of metabolic and anatomical imaging provides superior diagnostic capabilities in certain clinical situations – above all, for cancer.
PET: 18F-FDG and tumour response
PET has a uniquely high sensitivity, in the picomolar range, and uses radio-labelled tracers which provide molecular information for characterizing tumours and metastases. The tracers are injected in minute, non-pharmacological doses, and 3-D images are subsequently reconstructed by computer to show the concentration and location of specific tracers.
PET rapidly began to gain traction in the early 2000s, after it was realized that the imaging of specific molecular targets associated with cancer would permit earlier diagnosis and better management of oncology patients. A review published in 2002 foresaw PET becoming increasingly important in cancer imaging over the decade. Since then, PET has offered a way out of some of the key limitations in anatomical approaches for imaging cancer biology.
More recently, PET has begun to gain widespread acceptance for assessments of tumour response to chemotherapy and radiotherapy, when combined with the 18F-fluorodeoxyglucose (18F-FDG), glucose analogue. The commercial availability of the latter catalysed widespread introduction of PET in smaller hospitals and medical centres. Although quantitative analysis of 18F-FDG uptake is required for predicting tumour response early in therapy, according to some a visual interpretation of scans is often sufficient to assess response after the completion of therapy.
PET/CT seeks to address anatomical information deficit
PET images, however, still lack detailed anatomical information. An effort to address such a lack was to fuse PET data with high-resolution, three-dimensional morphological images from computer tomography (CT), which have been achieving sub-millimetre spatial resolution for well over a decade. Since the mid-2000s, PET examinations have indeed been performed in combination with CT and hybrid PET/CT systems have shown far greater accuracy in data registration from the two modalities than achievable by software fusion of separate images. The hybrid data has of course also proven to be of higher diagnostic value than either PET or CT on their own – apart from also simplifying the logistics of patient management. New PET installations are now almost exclusively comprised of combined PET/CT scanners
Key advantages of the combination, according to a 2009 study by Vanderbilt University Medical Center in the US include superior lesion detection, improvement in the localization of foci of uptake resulting in
The conventional method of prostate cancer detection is based on blood tests showing elevated prostate specific antigen (PSA) levels followed by an uncomfortable digital rectal examination (DRE) and a 12-needle biopsy under ultrasound guidance.
Professor Jelle Barentsz, Head of the Prostate MR Reference Centre in Nijmegen, Netherlands, has pioneered a novel approach using magnetic resonance imaging (MRI) to effectively confirm or exclude suspected prostate cancer as well as determine the aggressiveness and spread of the disease, and even treat it in a number of cases. Despite obvious advantages, this approach has yet to gain wider acceptance, not least among radiologists who need to be trained for the procedure. Insurance companies and national health systems also have to be convinced of the benefits of the MRI-based method.
The limitation of the standard PSA test is its low specificity

A 354-patient study on image quality and dose values for thorax images with the DX-D 300 digital radiography system and MUSICA 3 software was carried out at the Institute of Imaging Diagnostics and Therapy (BDI) in Erlangen. Dr. Karina Hofmann-Preiss, summarizes here the details and findings of the study.
Agfa HealthCare

Integrated patient care
It is helpful to have a goal, even in the knowledge that it can never be reached. Some enthusiasts in the Integrating the Healthare Enterprise (IHE) community, including myself, follow the road towards developing IHE integration profiles to reach the goal of an integrated patient care (IPC), see figure 1, even knowing that it means reaching for the impossible.
The eight components contributing towards IPC shown in figure 1 are not representative of healthcare in general, but may be seen in the context of decision making for patient-specific therapeutic approaches. The healthcare unit which typically plays a major role in the process of therapy decision making is the therapy planning unit or tumour board. Here, ideally, many information sources available about the patient (radiology, pathology, oncology, surgery, etc.) should be considered before subsequent diagnostic or therapeutic steps are being taken.
In a real clinical setting this means that a combination of quantitative and qualitative information about the patient has to be mentally integrated by the physician to create an abstract representation (model) of the patient. This model must be as close as possible to reality to serve as a basis for decision making in medical diagnosis and therapy.
Based on the model created in the physician

In spite of clusters of world class hospitals in high-end districts of major cities, the BRICS group of large emerging markets (Brazil, Russia, India, China and South Africa) are handicapped by rudimentary healthcare infrastructure in outlying regions and in their countrysides. In addition, even in central urban areas, the growth of new lifestyle diseases threatens to swamp existing facilities.
Prins Hendrikstraat 1
5611HH Eindhoven
The Netherlands
info@interhospi.com
PanGlobal Media IS not responsible for any error or omission that might occur in the electronic display of product or company data.
