


The European Respiratory Society (ERS) published their first White Lung Book a decade ago, to provide a comprehensive survey of respiratory health across Europe for the benefit of patients as well as medical personnel and policy makers. The book aimed to highlight the huge and underestimated burden of respiratory disease in the region. Since then political and economic upheavals as well as an expansion in medical research and development have necessitated a second edition of this invaluable book, which was published ahead of this year

The very first intensive care units (ICUs), introduced towards the end of the 19th century, consisted of a few beds reserved for the sickest patients and put together in one area of the general hospital ward so that the patients could be watched more closely. Patients continued to be treated by their admitting physician with consultation by other specialists as dictated by the course of their disease. Later, separate rooms were created to gather together the special monitoring and organ support equipment and specially trained nursing and medical staff considered necessary for the optimal management of critically ill patients.
Over the years, especially in larger hospitals and more commonly in the United States than in other countries, subspecialty ICUs have developed, catering for specific groups of patients, such as those with neurological, respiratory, cardiac, surgical, trauma diagnoses. This division of intensive care into subspecialties reflects a general trend across medicine towards the creation of increasingly specialized subspecialties. In the United States, one third of all ICUs are now (sub)specialty units. But is there any evidence that such units provide better care than general, multidisciplinary ICUs catering for all critically ill patients regardless of diagnosis?
by Prof. Jean-Louis Vincent
Benefits of subspecialty ICUs
Proponents of specialized ICUs suggest that patient outcomes can be improved in such units because they are managed by staff with increased expertise and training in the particular field of diagnosis. Such units are thus able to provide more focused, relevant care. However, although highly trained in their particular specialty, staff in such units may be less experienced in diagnosing and managing other systemic complications of critical illness. There is relatively little data available comparing the benefits of specialty versus general ICUs. In one study, patients with intracerebral hemorrhage had improved survival rates when admitted to a specialized neurosurgical ICU compared to a general ICU [1]. However, in another analysis, admission to a diagnosis-appropriate specialty ICU was associated with no survival benefit compared to admission to a general ICU for a selection of common diagnoses, including acute coronary syndrome, ischemic stroke, intracranial hemorrhage, abdominal surgery, and coronary-artery bypass graft surgery [2]. Interestingly, admission to a diagnosis-inappropriate specialty ICU, e.g., a renal patient admitted to a neurosurgical ICU because the renal ICU was full, was associated with increased mortality rates [2]. Performing such comparative studies is, however, fraught with difficulty, largely because there is no set definition of a


COCIR (European Co-ordination Committee of the Radiological, Electromedical and Healthcare IT Industry) has just released their third edition of its annual report on the Self-Regulatory Initiative (SRI) on the ecodesign of medical devices. The Initiative has been supported and officially acknowledged by the European Commission at the end of 2012.
The COCIR committee was founded in 1959 as a voice for the medical technology industry in Europe with members consisting of key players in the development of healthcare in Europe and worldwide. They seek to promote the development of harmonized international standards and regulatory control respecting the quality and effectiveness of medical devices and healthcare IT systems, without compromising the safety of patients or users. One of the main goals of COCIR is to be pro-active in Green Technology (Eco-Design) and with this in mind the COCIR companies proactively committed with the European Commission to develop a self-regulatory initiative under the Echodesign Directive to reduce the environmental impact of medical imaging equipment. The project was presented to the European Commission in 2008. The first version of the SRI methodology was submitted for comment during 2009 which led to the submission of a new SRI 2 methodology to the EU Commission in February 2012. During November 2012, the commission acknowledged the initiative recognizing the benefits for society and healthcare. Each year a Status Report is published reporting on the progress and achievements of the initiative. This report is the third annual SRI Status report, the first after acknowledgement of the European Commission. The current status report has focused on CT (computer tomography), after having covered ultrasound and magnetic resonance modalities in 2010 and 2011 respectively.
Based on a consensus reached among themselves on a set of ecodesign targets, COCIR
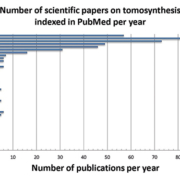
X-ray based imaging techniques include a variety of different implementations and applications: computed radiography (CR), digital radiography (DR) and variations of computed tomography (CT): clinical CT, C-arm, tomosynthesis, micro-CT, industrial CT. These X-ray based methods are widely used not only for diagnostics and assistance in clinical practice but also for screening in security applications and for non-destructive material testing in industry, archeology and material science. The aim of this review paper is to give an introduction into a modern X-ray based tomographic imaging technique, called Digital Tomosynthesis (DT). DT is known as an attractive low-dose alternative to CT in medical (and non-medical) imaging applications.
by Yulia M. Levakhina, Thorsten M. Buzug
Historical overview: from radiostereoscopy to digital tomosynthesis
The history of X-ray imaging starts in 1985 when Wilhelm Conrad Roentgen discovered a new kind of radiation which he called X-rays. It was a breakthrough invention that allowed visualization of inner structures of the human body without surgical intervention.
Analogue imaging
A simple radiographic image contains the superposition of all three-dimensional structures in an object as a two-dimensional image. This means that is it impossible to recover the depth of information of any particular feature (e.g. tumour). At the beginning of the 1920s there were many attempts to erase superimposed shadows from X-ray images and to benefit from the use of X-rays for imaging of the human body. Owing to the fact that the communication between researchers from different countries was very limited at that time, many scientists were re-discovering similar imaging concepts. It resulted in a number of patent applications and scientific papers, which all discussed the same imaging technique where the X-ray tube and X-ray receptor move in parallel planes. The result of each acquisition was an analogue image showing sharply the only one plane located in focus while blurring all other planes. This technique was called stratigrafia by A. Vallebona, planigraphy by A. E. M. Bocage and B. G. Ziedses des Plantes or laminography by J. Kieffer. More information can be found e.g. in the historical article written by a curator of the Belgian Museum of Radiology, R. van Tiggelen.
Digital tomosynthesis or computed tomography?
The next step forward was the implementation of a device, where each measured radiographic image can be stored separately and processed after the examination instead of integrating the measurements directly on film. By doing this, it is possible to generate an arbitrary number of planes or laminograms through the object based on the limited number of measured radiographs. The total radiation dose can be reduced because only one examination is needed to produce images of the whole volume. This is essentially the main idea of modern tomosynthesis as it is known today. The word tomosynthesis was introduced by D. G. Grant in 1972. A number of further improvements of tomosynthesis, mainly focused on improving image quality and shortening acquisition time, have been proposed during the 1970s and 1980s. The review papers by Dobbins give a detailed overview of tomosynthesis research during the 1970s and 1980s.
In that same year (1972), there was an another development when Sir Godfrey Hounsfield and James Ambrose gave a talk on

Data sharing between healthcare organizations can improve clinical efficiency and enable better decision-making. This is essential at a time when health services in Europe are facing perhaps their greatest challenge to date. Providers must accommodate increasing demand for services due to ageing populations, the rising prevalence of chronic diseases and budgets being constrained. The ability to compare costs to benchmarks will be crucial for healthcare providers needing to maintain or improve standards of care and achieve cost reductions and efficiency targets without cutting frontline staff. However, it will be necessary to look at key performance indicators (KPIs) more from a clinical achievement perspective than an operational cost or activity-based perspective. Data collection and dissemination will also be central to achieving these aims, as hospitals and providers adopt a more collaborative and integrated approach to healthcare.
by Peter Osborne
Growth in healthcare spending per capita has slowed or fallen sharply in real terms in almost all European countries since 2010 [see Figure 1]. Previous to the economic crisis, it had been rising faster than the rest of the economy, according to the European Commission (EC) and Organization for Economic Co-operation and Development (OECD).
As a result, there is a pressing need to change the way healthcare services are commissioned and delivered. Although national health systems in Europe are diverse, with models varying from predominantly single payer health services, to systems of competing insurers and providers, there is a growing recognition that advanced analytics employed at every point of care will play a key role in advising on how to move forward.
According to analysts at Frost & Sullivan, hospitals and other healthcare providers will need to invest in advanced data analytics solutions to monitor end-to-end care delivery across a variety of settings, as well as provide comprehensive reporting on performance and quality measures to a variety of stakeholders.
Up until recently however, the healthcare sector has suffered from disjointed approaches to collecting data, with highly-fragmented systems used by various payers, providers, and government agencies. Furthermore, many have yet to adopt any form of analytical approach to the clinical, financial and administrative data they collate.
A recent Accenture survey of 3,700 physicians across eight countries globally found that the main barriers to health information exchange were: IT systems that are unable to

The World Hospital Congress is an initiative of the International Hospital Federation (IHF), re-established in 1947 and based in Geneva. IHF is an international non-governmental organization supported by members from over 100 countries. Last June, the 38th edition was held in Oslo, Norway and the Norwegian Hospital and Health Services Association (NSH), a member of IHF, was involved in the organization of the 3-day event.
International Hospital talked to Dr Bernadette Kumar, NSH board member and president of the International Scientific Committee piloting the conference programme, about the scope of this important meeting for hospitals around the world.
Q. The 38th World Hospital Congress was successful in attracting a large number of delegates as well as high level speakers such as Dr Margaret Chan, WHO Director. As member of the Norwegian Organizing Committee and President of the Scientific Committee, can you tell us about the main challenges of putting together an event of such scope? Are there any pitfalls to be avoided?
The first key lesson is that there are never any shortcuts to success; it takes a lot of hard work, time and effort not only of an individual or key persons but a good team in putting together a good programme. Norway as a country has been known to box in a class higher than its own and it is this spirit of aiming high and for the best that secured high level speakers such as Dr. Chan. To quote one of the participants based on the evaluation, the Plenary sessions were outstanding!
Oslo 2013 clearly reflects the handiwork of a highly competent and dedicated team. Teamwork required both resilience and persistence; never giving up despite disappointments, shortcomings and even though the process could be both time consuming and tedious.
It is an extremely daunting task to satisfy and meet the needs of such a multidisciplinary global audience. Thus the main challenge of putting together such an event is striking the balance, the programme has to be relevant and interesting for a board range of subjects and a multidisciplinary audience. The programme has to cater for wide participation and in meeting the needs of all there is a danger of spreading the programme too thin. There has to be something for everybody but not everything on the programme will appeal to all participants. So the pitfall to be avoided is a highly specialized programme, but at the same time if it is too general it will not generate sufficient interest or satisfy the needs.
Q. One of the important themes discussed was the role of technology and innovation in improving the delivery and effectiveness of healthcare. There seems to have been varied and sometimes contrasting views on this key issue, could you briefly touch upon the most important points that were made? Is there a take home message on this essential question?
We live in the age of technology and healthcare is no island. Technology and innovation have serious implications for future healthcare. Technology has consequences for healthcare and despite the difference in viewpoints one thing is certain; that it cannot be ignored. Oslo 2013 provided a platform that shed light on the consequences of technology for healthcare, the challenges and ethical dilemmas technology poses. Furthermore, the positive results were shared and discussed and last but not the least the sharing of experiences from around the around the globe and learning from one another enhanced the air of optimism. The participants appreciated the possibility to gain insight as to the state of the art from both the North and South. The North South dichotomy is well known and notwithstanding the great variation in resources there are similarities especially with regards to the challenges. Dr. Margaret Chan said
Prins Hendrikstraat 1
5611HH Eindhoven
The Netherlands
info@interhospi.com
PanGlobal Media IS not responsible for any error or omission that might occur in the electronic display of product or company data.
