


The use of ultrasound for diagnostic imaging has grown by leaps and bounds in recent years and is now the preferred approach for many applications, but according to experts the application with the biggest growth potential is imaging of the musculoskeletal system.
Major developments in the technology, which now provides a number of modes including grey scale, colour and power Doppler, spectral Doppler and elastography, allow accurate characterization of joint pathology; even the acquisition of dynamic, essentially isotropic 3D images is now possible. The biggest remaining challenge is reported to be the adequate training and monitoring of medical professionals to enable them to carry out this highly complex ultrasound application.
However, while patients ranging from young athletes with suspected torn tendons, muscles or ligaments to those suffering from chronic conditions such as rheumatoid arthritis or osteoporosis
Partial support for patients with respiratory failure can be provided with invasive mechanical ventilation or non-invasive mechanical ventilation. The role of non-invasive positive pressure ventilation (NPPV) in preventing intubation for various conditions has been well studied. Less well studied is the role for NPPV in the weaning and peri-extubation period.
by Dr Brooks A. Fallis and Dr Karen E. A. Burns
Mechanical ventilation is essential for supporting patients through episodes of respiratory failure by unloading respiratory muscles and improving gas exchange. While potentially lifesaving, invasive mechanical ventilation with an endotracheal tube or tracheostomy can be associated with important harm, in part due to complications such as ventilator associated pneumonia (VAP). VAP has been shown to increase morbidity and trends towards increasing mortality [1].
Critical care physicians strive to extubate patients as early as possible, while minimising the risk of re-intubation, which has been shown to be independently associated with increased risk of developing VAP [2]. Spontaneous breathing trials (SBT) are used to decide if a patient has been weaned. An SBT involves a focused assessment of a patient

Given their pervasiveness in hospitals, one could be forgiven to take picture archiving and communication systems (PACS) for granted. However, in reality, they have been around for less than two decades. The first PACS prototype was set up in 1990 at the University of California, and soon after at Hammersmith Hospital in London. Commercial products began to enter the market 3-4 years later but serious growth in PACS use was seen only in the early 2000s.
PACS: boost to productivity and imaging demand
PACS revolutionized workflow between radiology and other hospital departments, resulting in a gigantic leap in productivity. PACS also catalysed the growth of imaging, especially computed tomography (CT) and magnetic resonance imaging (MRI) scanners, whose huge masses of data it was able to process, store and forward to different users on demand.
Along with older X-Rays and ultrasound (whose data are also managed by PACS), CT and MRI devices have become integral to nearly every single surgical procedure, as well as the medical management of chronic diseases ranging from arthritis to cancer. In acute care settings such as A&E, their availability has directly contributed to a fall in patient waiting times and increased the efficiency of triaging.
2007: 3D video of beating heart
Until recently, 2D PACS was the only realistic choice. In spite of an explosion in core processing power and storage capacity, PACS technologies had been consistently outpaced by developments in CT, which permitted imaging of increasingly thinner slices, outputting exponentially larger volumes of data.
In 2007, Toshiba launched Aquilion One, with a capability of acquiring five 320 slices per second and attaining a highly-symbolic milestone
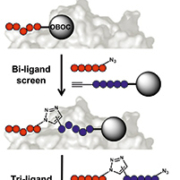
There is a growing need for affinity agents for targeted molecular imaging of disease biomarkers. Protein catalysed capture agents (PCC agents) are assembled through target-guided in situ click chemistry and display low nanomolar affinity and specificity. The iterative design process, architecture, and composition of the resulting multi-ligands make this a promising technology for imaging agent development.
by Dr Steven W. Millward, Dr Heather D. Agnew, Dr Suresh Pitram, Dr Bert T. Lai, Dr Rosemary D. Rohde and Dr Norman Hardman
Personalized medicine is increasingly becoming a major component of cancer treatment and management. Many of the advances in personalized medicine have come from high throughput genomic sequencing and multiplexed proteomic analysis of tumour and tissue specimens. While these technologies have dramatically increased our understanding of cancer and cancer heterogeneity at the molecular level, translation of this knowledge into clinical imaging agents to non-invasively characterize tumour phenotypes in vivo has lagged behind. While small molecules (e.g. FDG) have proven very useful for clinical measurement of metabolic activity, molecular imaging of cell surface and secreted biomarkers overexpressed in cancer (e.g. IGFR, EGFR, etc.) is largely confined to the preclinical and early clinical trial setting.
While groundbreaking work to determine the biological and therapeutic roles of these proteins has produced a wealth of high affinity antibodies, antibody fragments, and peptides, attempts to translate them into radiotracers for molecular imaging have produced mixed results. Antibody-based imaging agents suffer from three disadvantages in this setting:
1) Their long serum half-lives, while advantageous for therapeutic applications, result in high background signal in perfused tissue and lengthen the time between agent administration and image acquisition.
2) Antibody-based radiotracers often show accumulation and metabolic processing in the liver, increasing nonspecific signal and potentially obscuring critical tumour-specific signal in the abdominal cavity.
3) Antibodies are biologicals, and as such their high production costs and regulatory burdens are significant economic barriers to commercialization and clinical translation. Linear peptides derived from phage display represent a second class of potential imaging agents, however their rapid degradation in vivo typically results in nonspecific background signal and poor tumour uptake. An ideal targeted molecular imaging agent would combine the affinity and specificity of antibodies with the high bio-stability, tumour uptake, and clearance of small molecules.
PCC agent design
Protein catalysed capture (PCC) agent technology represents a novel approach to rapidly design ligands with high affinity and specificity that can be potentially adapted to a variety of research and in vivo clinical applications including molecular imaging. This technology was built upon the observation by K. Barry Sharpless and co-workers at The Scripps Research Institute that the azide-alkyne cycloaddition (a
CT scans produce high resolution, three-dimensional (3D) images routinely used in medical diagnostic and image guidance procedures. The rapid advances in CT, including faster acquisition times and enhanced tissue discrimination capabilities, have also led to a broader range of applications for CT. Recently, however, there has been increased concern regarding the radiation dose received by patients during CT scans. Risks due to radiation are present because CT generates 3D images from a set of X-ray radiographs (or projections), which are recorded at different angles as the X-ray source rotates about the patient.
by Steven Bartolac and Dr David Jaffray
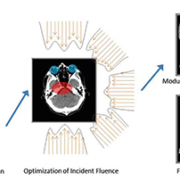
The concerns regarding radiation have been largely stimulated by a number of publications produced over the last five years that have indicated that the number of CT scanning procedures is on the rise (on the order of about 10% per year [1]), and that the increased risk of cancer due to radiation doses received from CT scans may be non-negligible [2], especially in patients receiving multiple CT scans [3]. Motivated by these concerns, fluence field modulated computed tomography (FFMCT) has been proposed as a new approach for CT imaging that promises better management of dose to the patient [4-6] without sacrificing image quality [See Fig. 1].
The tradeoff between image quality and radiation exposure
Though image quality is dependent on many factors, including image blur, and distortions that can arise from poor modelling of the X-ray physics, image noise is often a key determinant of image quality and the utility of CT scans, and is most directly related to the imaging dose. Image noise refers to random fluctuations in the image, which, when large, can obscure the details of interest. In CT images, the largest source of noise is due to inherent statistical fluctuations associated with photon counting (i.e. Poisson noise). The magnitude of this noise is inversely proportional to the average number of photons that reach the detector. Increasing the number of incident photons, or the X-ray fluence (i.e. photons/unit area) can help limit noise in the image but also results in increases in dose. Conversely, attempting to reduce the dose is associated with increased noise. Managing this tradeoff requires choosing the most appropriate scan settings considering the imaging task, and individual factors including patient age and size.
Conventional strategies for dose management
Non-uniformity of noise in CT images (i.e. image noise which changes in magnitude at different positions within the image) occur because different regions of the patient attenuate the X-ray fluence to varying degrees. Generally, a longer path length through the patient suggests greater attenuation of the beam, and greater noise associated along that X-ray path. If the patient is modelled as an elliptic cylinder, the path length is longer near the centre of the patient than near the periphery. To compensate for these changes, bowtie filters are typically included in conventional scanners to limit the incident fluence at the peripheries of the patient and allow higher fluence near the centre, creating a more uniform exposure at the detector. In this way, overexposure to the peripheries is prevented when attempting to limit noise near the centre of the patient. In the elliptical model, some views of the patient are also more greatly attenuating than others. Tube current modulation (TCM) is therefore used in conjunction with bowtie filters, which allows the overall fluence to be increased or decreased depending on the view. [See Fig. 2 for schematic illustrations of bowtie filtration and TCM.]
FFMCT: a new paradigm for CT imaging
Though bowtie filters and TCM greatly aid in decreasing dose to patients, patient anatomy is inherently more complex than the representation by a simple elliptical shape. The presence of bony and lung tissue, for example, introduces large variations in beam attenuation across the field of view. The pattern of beam attenuation also depends greatly on the incident angle of the X-rays. Contrary to conventional approaches that use a fixed filter in place throughout the scan, FFMCT proposes to use a dynamic modulator allowing the fluence to change freely across the field of view and for different projection angles, such that each projection may have a distinct incident fluence pattern [See Fig. 1].
Increased flexibility in the delivery of X-ray fluence suggests better management of dose since higher exposures can be reduced where not required for maintaining the desired image quality. In the proposed methodology for FFMCT, an input model of the patient could be used to define an image quality plan defining the desired image quality for the given task [See Fig. 1]. The plan could further define specific regions where low dose is a priority. An optimization algorithm can then be used to search for a modulation pattern that comes as close to the planned objectives as possible. As many patients undergo multiple CT scans, a previous CT scan could potentially be used as the model; alternatively, a population based model could be used.
Achieving task-based, user-defined image quality
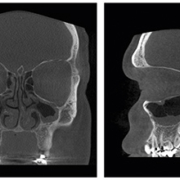
In many cases, the desired image quality may vary within the image. For example, one might desire higher image quality in a small region of interest (ROI) near a suspicious lesion in a repeat CT scan; in another case, one might only be interested in the region of the heart in a cardiac CT scan; in an image-guided surgical procedure, the ROI may be restricted to a localized region surrounding a surgical instrument. In these cases, allowing the image quality to be reduced outside the ROI may be advantageous, since it suggests a reduction in total dose to the patient. Initial research [5, 6] has suggested that fluence modulation patterns can be found that allow for better uniformity of image quality in target ROIs than afforded by conventional means, while allowing for image quality elsewhere to be reduced. [See Figs. 3 and 4.]
Dose reduction
The amount of dose reduction possible compared to conventional approaches using fluence field modulation depends highly on the patient and the task. Preliminary research using a simulated thorax phantom [5, 6] suggests that integral dose reduction across a single image slice (in Joules) could range up to 50% or higher for applications where the region of interest is well localized [5]. Local dose reductions (in cGy) outside the ROIs can approach 60-80%. Research is ongoing for evaluation of dose benefits to other sites.
Technology advances towards FFMCT
Currently, no device has been introduced in modern scanners that can offer the unconstrained, flexible modulation patterns proposed for fluence field modulation. Design challenges include speed demands on dynamic modulators given the very rapid gantry speeds of conventional scanners, and changes to the energy spectrum of the incident beam that might occur as a by-product of modulation using a dynamic filter. However, several simplified approaches for modulator designs have been proposed that make significant steps towards achieving fluence field modulation in clinical scanners, including a series of sliding wedges [7], dynamically moving discrete apertures [8, 9], and multiple sources in inverse geometry CT [10] (e.g. the

In the days of film-on-a-lightbox, dose seemed easier to control. If you overexposed film, the image would turn black. It you underexposed, the image would be too light. These technical realities exercised subtle control over the range of dose that would produce a useable image. With the advent of digital imaging, those subtle nuances have changed.
Digital dose creep
Technologists soon learned that slight overexposure in digital imaging could create a better looking image. So there was a natural tendency for doses to slowly edge higher in the name of image quality. Add to this the steady increase of new types of modalities coming on line and the patient
Ergonomics is the use of design to achieve greater productivity and safety, and has long had special significance in the healthcare area. Though usually defined as a science, healthcare ergonomics embodies a strong element of art too: the key reason is the impact of the (unquantifiable) patient
Prins Hendrikstraat 1
5611HH Eindhoven
The Netherlands
info@interhospi.com
PanGlobal Media IS not responsible for any error or omission that might occur in the electronic display of product or company data.
