

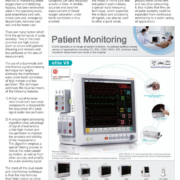
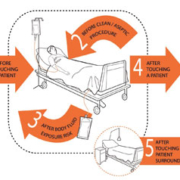
Hand hygiene is a crucial part of patient safety in healthcare settings. Hand hygiene promotion using a multimodal strategy incorporating alcohol-based handrub is now the standard of care. A wealth of information and practical tools are available through the World Health Organisation

In the interviews published in International Hospital we focus on a particular field of expertise to find out about the current developments. We spoke to Dr Jean-Louis Brasseur, consultant at Piti

From Epidemiology and Immunobiology to a Rational Diagnostic and Therapeutic Approach

Patients are at risk of infection from the numerous types of pathogens that can survive in hospitals. The cleaning process could have a huge impact on this risk if it is aimed at the most frequently contaminated sites, removes or kills viable organisms and is carried out sufficiently frequently to inhibit accumulation of pathogens. Whilst there are an increasing number of products on the market to facilitate the cleaning process, evidence of their efficacy is needed. Frequent detergent-based cleaning also requires urgent appraisal in order to compare alternatives for cleaning hospitals.
by Dr Stephanie J. Dancer
More evidence is accumulating for the role of cleaning in controlling infection in hospitals. There are a variety of hardy hospital pathogens such as meticillin-resistant Staphylococcus aureus (MRSA), vancomycin-resistant enterococci (VRE), norovirus, Acinetobacter and Clostridium difficile, all of which can persist in healthcare environments for considerable lengths of time. Basic cleaning can help in the control of these pathogens, usually as part of an overall package in response to an outbreak, but there is also a role for enhanced cleaning in the non-outbreak situation. Organisms on hand-touch sites in hospitals are thought to provide the most important risk for transmission because hand contact with a contaminated site could deliver a pathogen to a patient. However, current cleaning regimens do not necessarily target high-risk reservoirs and there remains confusion between nursing and domestic personnel over allocation of cleaning responsibilities. Whilst there is little evidence for the most effective cleaning frequencies, some sites do not receive the cleaning attention that they deserve. Thus, cleaning practices should be tailored to clinical risk, as well as reflect the wide-ranging surfaces, equipment and building designs in today
The number of peer-reviewed papers covering the field of ultrasonography is huge, to such an extent that it is frequently difficult for healthcare professionals to keep up with the literature. As a special service to our readers, IHE presents a few key literature abstracts from the clinical and scientific literature chosen by our editorial board as being particularly worthy of attention.
Heart failure secondary to dilated cardiomyopathy: a role for emergency physician bedside ultrasonography.
Heart failure as a result of cardiomyopathy is an uncommon presentation in the pediatric emergency department (PED). The initial presenting symptoms in these cases are often nonspecific and may be confused with more common paediatric illnesses. This article reports the case of a 3-year-old girl initially discharged from a PED after routine evaluation of vomiting and diarrhoea with a diagnosis of acute gastroenteritis, only to return one week later in heart failure from a dilated cardiomyopathy. A bedside ultrasound performed by the emergency physician in the PED allowed for the initiation of appropriate, rapid, goal-directed therapy and expedited timely transport to a facility with paediatric cardiothoracic surgery. Dilated cardiomyopathy and the role of emergency physician echocardiography is reviewed.
The validity of ultrasonography in the diagnosis of zygomaticomaxillary complex fractures.
This study determined the sensitivity, specificity, positive and negative predictive values of ultrasonography in detecting zygomaticomaxillary complex fractures, and highlighted factors that may affect the validity of ultrasonography in these diagnoses. Twenty-one patients with suspected fractures of the zygomaticomaxillary complex were included in this prospective study. All the patients had plain radiographic and computed tomography (CT) investigations. All underwent ultrasonographic examination of the affected region using an ultrasound machine with a 7.5MHz probe. The different radiologists were not aware of the results of the other two investigations. Statistical significance was inferred at P<0.05. The validity of ultrasonography varied with fracture sites with a sensitivity of 100% for zygomatic arch fractures, 90% for infraorbital margin fractures and 25% for frontozygomatic suture separation. Specificity was 100% for the three types of fracture. There was no statistically significant difference in the ability of CT and ultrasonography to diagnose fractures from various zygomaticomaxillary complex fracture sites (P=0.47). Ultrasonography appears to be a valid tool for the diagnosis of zygomatic arch and displaced infraorbital margin fractures. Imaging inflammatorybreast cancer.
Carcinomatous mastitis is a severe form of breast cancer and its diagnosis is essentially clinical and histological. The first examination to perform is still mammography, not only to provide evidence supporting this diagnosis but also to search for a primary intramammary lesion and assess local/regional spread. It is essential to study the contralateral breast for bilaterality. Ultrasound also provides evidence supporting inflammation, but appears to be better for detecting masses and analysing lymph node areas. The role of MRI is debatable, both from a diagnostic point of view and for monitoring during treatment, and should be reserved for selected cases. An optimal, initial radiological assessment will enable the patient to be monitored during neoadjuvant chemotherapy.
Current role of ultrasound in chronic liver disease: surveillance, diagnosis and management of hepatic neoplasms.
Despite certain inherent limitations in evaluating chronic liver disease on routine gray-scale US, it is still widely used for the initial evaluation in patients suspected of liver disease as well as for hepatocellular carcinoma (HCC) screening in patients with known cirrhosis. Due to recent advances in digital technology and US imaging software, various new computer protocols have been incorporated in the new US equipment. This in turn has resulted in a great improvement in image quality and image resolution. Consequently, the increased ability of US to better characterise the liver texture in general has enabled sonographers to identify subtle changes in the liver texture and delineate smaller masses in the liver with greater success.
Prins Hendrikstraat 1
5611HH Eindhoven
The Netherlands
info@interhospi.com
PanGlobal Media IS not responsible for any error or omission that might occur in the electronic display of product or company data.
