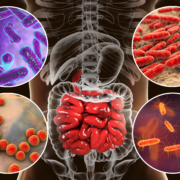
CN Bio, a leading organ-on-a-chip company (OOC) that designs and manufactures singleand multi-organ microphysiological systems (MPS), has secured the licensing rights to a novel tool for modelling the gut microbiome, GuMI, from Massachusetts Institute of Technology (MIT) and North-eastern University. Planned for commercial launch in 2023, the technology will be integrated into CN Bio’s PhysioMimix […]
https://interhospi.com/wp-content/uploads/sites/3/2021/09/shutterstock_1031178730-1-scaled.jpg17072560panglobalhttps://interhospi.com/wp-content/uploads/sites/3/2020/06/Component-6-–-1.pngpanglobal2021-09-21 12:29:482021-09-21 12:41:17CN Bio licenses human gut microbiome modelling tool from MIT and Northeastern University
Ashikaga Red Cross Hospital, Japan’s first green hospital
Leaders of the global healthcare community are invited to attend an important virtual event looking at developing innovative practices for a sustainable future.
It will bring together hospital executives from around the world to share their strategies and experiences in promoting sustainability in the healthcare sector.
Climate change – a major threat to public health
Hospital and healthcare professionals are at the forefront of the fight against climate change, which is at risk of becoming the biggest public health threat of our generation:
If the world’s healthcare sector were a country, it would be the fifth-largest emitter of carbon emissions on the planet.
Medical professionals have identified climate change from carbon emissions as the ‘biggest global health threat of the 21st century’. (The Lancet, Commission on Climate Change, 2009)
Between 2030 and 2050, climate change is expected to cause more than 250,000 additional deaths per year.
Dr. Satoru Komatsumoto, Emeritus Director of Ashikaga Red Cross Hospital, will share his insights into designing a resilient hospital.
The keynote speaker at the event will be Dr. Satoru Komatsumoto, Emeritus Director of Ashikaga Red Cross Hospital, which is Japan’s first green hospital Dr. Komatsumoto will share his insights into designing a resilient hospital.
He commented: “Sixteen years ago, I proposed that our hospital should be eco-conscious. I wanted to create a hospital that would be beautiful and that would organically integrate all the features to meet the challenges of the future… I wondered what kind of hospital would meet the needs of our time. I studied very hard to imagine a next generation hospital.”
The program also includes speakers from Europe and the USA who will share strategies to achieve net zero carbon emissions by 2030, sustainable food circuits and building a carbon-neutral hospital. There will also be dedicated time for small group discussions with the experts to explore innovative ideas.
You can register here for Green Hospitals: Sharing innovative practices for a sustainable future.
https://interhospi.com/wp-content/uploads/sites/3/2021/09/Komatsumoto_web.jpg790770panglobalhttps://interhospi.com/wp-content/uploads/sites/3/2020/06/Component-6-–-1.pngpanglobal2021-09-13 10:30:282021-09-13 10:30:28Join the Green Hospitals event to develop innovative practices for a sustainable future
Thomas Korn, professor of experimental neuroimmunology at TUM
Scientists have long been aware of a link between the gut microbiome and the central nervous system (CNS). Until now, however, the immune cells that move from the gut into the CNS and thus the brain had not been identified. A team of researchers in Munich has now succeeded in using violet light to make these migrating T cells visible for the first time. This opens up avenues for developing new treatment options for diseases such as multiple sclerosis (MS) and cancer.
The link between the gut microbiome and the CNS, known as the gut/brain axis (GBA), is believed to be responsible for many things: a person’s body weight, autoimmune diseases, depression, mental illnesses and Alzheimer’s disease. Researchers at the Technical University of Munich (TUM) and LMU University Hospital Munich have now succeeded in making this connection visible for the first time. This is cause for hope – for those suffering from MS, for example. It may offer ways to adapt treatments, and T cells could perhaps be modified before reaching the brain.
Immune cell migration in MS
The immune system is affected by environmental factors – also in the central nervous system in case of MS patients. This autoimmune disease is subject to repeated flare-ups, experienced by patients as the improvement or worsening of their condition. T cells collect information and, in MS patients, carry it to the central nervous system (in the brain or spinal cord) where an immune response is triggered. Until now, however, it was long uncertain how and from where the T cells were travelling to the CNS
Using violet light to track marked T cells
The team working with Thomas Korn, a professor of experimental neuroimmunology at TUM, has developed a method for marking immune cells in mice using photoconvertible proteins. The T cells can then be made visible with violet light. The researchers successfully tested this method with the mouse model in lymph nodes, both in the gut and the skin. They were able to track the movement of the T cells from those locations into the central nervous systems.
Characteristics of T cells reveal their origin
T cells from the skin migrated into the grey and white matter of the CNS, while almost all T cells from the gut ended up in the white matter. For T cells in the brain, it was still possible to determine their origin.
“What makes these insights so important is that they demonstrate for the first time that environmental influences impact the T cells in lymph nodes in the gut and the skin, which then carry this information into the distant organs,” said Prof. Thomas Korn. “The characteristics of the T cells are sufficiently stable for us to determine whether immune responses are influenced by skin or gut T cells,” added LMU researcher Dr. Eduardo Beltrán, who performed the bioinformatic analyses in this study.
Starting point for future treatments
Michael Hiltensperger, first author, remarked that the research provided an important insight for MS patients: “If gut or skin cells were known to be the cause, the T cells could be treated at the source of the disease and predictions could be made on the progress of the chronic inflammation and autoimmune condition. The results of the study could also mean a breakthrough for research on other autoimmune diseases or cancer.
Reference:
Hiltensperger, M., Beltrán, E., Kant, R. et al. Skin and gut imprinted helper T cell subsets exhibit distinct functional phenotypes in central nervous system autoimmunity. Nature Immunology 22, 880–892 (2021). https://doi.org/10.1038/s41590-021-00948-8
https://interhospi.com/wp-content/uploads/sites/3/2021/09/t_cell_research_web.jpg9451417panglobalhttps://interhospi.com/wp-content/uploads/sites/3/2020/06/Component-6-–-1.pngpanglobal2021-09-07 10:17:392021-09-07 10:17:39Researchers observe for first time T cells travelling from gut to central nervous system
The 23rd National Healthcare CXO Summit will take place on 24-26 October 2021 in Boston, MA. This summit gathers leading healthcare executives and innovative suppliers and solution providers physically together at a premium location, the Boston, Encore, Boston, MA.
The summit effectively unites experts in an exclusive networking environment providing the opportunity to pre-schedule one-to-one physical business meetings with leading and forward-thinking executives. Delegates that have attended in the past include:
Beacon Health System – Chief Executive Officer
Elmhurst Hospital – President and Chief Executive Officer
Erlanger Health System – Executive VP and CFO/Treasurer
Luke’s Health System – President and Chief Executive Officer
Yale New Haven Health System – Executive Vice President/Chief Strategy Officer
The MetroHealth System – President and Chief Executive Officer
Mercy Health – Regional President and Chief Executive Officer
The one-to-one business meetings provide access to the gate keepers of sizeable budgets – top executives actively seeking external partnerships with operational, management, financial and technology solutions, geared entirely to the needs of healthcare industry.
https://interhospi.com/wp-content/uploads/sites/3/2021/09/CXO_summit_web.jpg6271200panglobalhttps://interhospi.com/wp-content/uploads/sites/3/2020/06/Component-6-–-1.pngpanglobal2021-09-02 11:19:222021-09-02 11:19:2223rd National Healthcare CXO Summit set for October in Boston
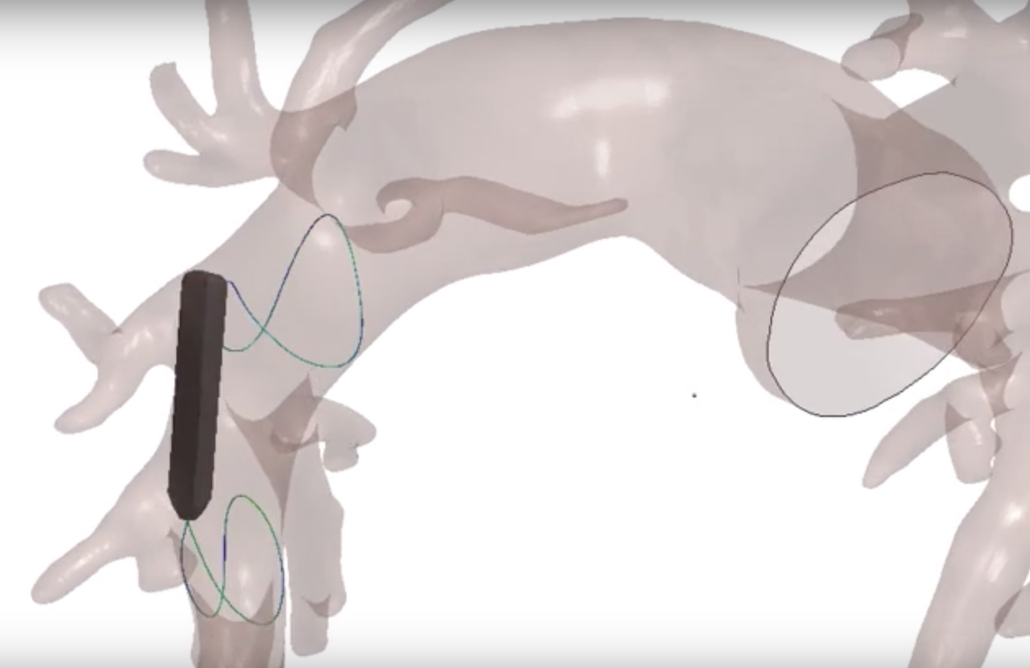
What if a computer simulation model of the heart and blood vessel could reduce the need for human or animal data in clinical trials, while speeding up product development? Biotronik and their research partners are looking into exactly that question in the new EU-funded SIMCor project. One of the first likely developments from this partnership will be an implantable sensor to better manage heart failure.
More than 10 million people in Europe suffer from heart failure. Beyond its obvious impacts on patient quality of life, treating heart failure uses 1-2% of a developed country’s health budget every year, with two-thirds of that taken up by hospital stays. If we can help reduce hospital visits related to heart failure, we can both help heart failure patients live better lives and reduce overall healthcare costs. That’s just one reason why Biotronik is taking part in SIMCor, a three-year EU-funded project to develop an implantable pressure sensor that aims to help heart failure patients and physicians better manage their condition.
Along with Biotronik, SimCor includes 11 partners from eight countries, including Berlin’s Charité Hospital. By pooling resources and data, SIMCor’s goal is to speed up the development of this technology and achieve results as fast as possible.
Beyond a new and innovative technology to support heart failure patients, the SIMCor partnership also has the potential to provide even longer-lasting benefits. If successful, computer simulations of the heart-implant interaction could speed up product testing and regulatory approval, providing many patients with technology that can save and improve their lives in a more timely manner.
How the SIMCor partnership can speed up the development process
The SIMCor project focuses on developing computer simulation technology that can help test and validate medical devices. These computerized tests could replace the need for animal testing and help make clinical studies even safer for patients. If a large and high-quality dataset is available, researchers can simulate clinical interventions in virtual patient cohorts. Over the longer term, this could reduce clinical trial size by 25%, with 30% less time required to complete studies. In the end, this allows medical devices to be quickly approved to help patients. The US FDA has already noted the potential positive effects such modelling could have, and is encouraging the development of simulation technology. By working together, Biotronik and its SIMCor partners can conduct these simulations using far bigger datasets than would otherwise be available, yielding the sophisticated modelling required to simulate heart and blood vessels.
Dr. Torsten Luther, Director of Product Development for Delivery Tools, Leads & Accessories in R&D at Biotronik
“We need to demonstrate that implants perform well across the whole patient population. That’s a long and sometimes challenging process because patient anatomy can vary widely, especially due to diseases,” said Dr. Torsten Luther, Director of Product Development for Delivery Tools, Leads & Accessories in R&D at Biotronik. “Using a large data pool to simulate different parts of the cardiovascular system, such as the heart or pulmonary artery, allows us to test implant performance across a wide range of anatomies representing the whole patient population. We can then optimize our technology for everyone.”
Collaboration is an important driver for innovation
Research and development have always been a priority at Biotronik. Since developing the first German pacemaker in 1963, Biotronik has continued to pave the way for pioneering innovations. In its Berlin headquarters alone, one out of every five employees work in R&D, ensuring that medical technology keeps pace with the interests and needs of future patients and physicians.
By investing in clinical trials and initiating research projects, Biotronik seeks to address research gaps and offer practical treatment options.
Dr. Andreas Arndt, Team Lead R&D Sensors and SIMCor project coordinator at Biotronik
“The SimCor project is a great example of how we work together with like-minded partners from different industries as well as academic institutions across Europe. We profit from each other’s knowledge and together, we can make an impactful contribution to medical research. In this regard, I believe that collaboration can be a key driver for innovation,” said Dr. Andreas Arndt, Team Lead R&D Sensors and SIMCor project coordinator at Biotronik.
https://interhospi.com/wp-content/uploads/sites/3/2021/08/pulmonary-artery-simulation.jpg15302360panglobalhttps://interhospi.com/wp-content/uploads/sites/3/2020/06/Component-6-–-1.pngpanglobal2021-08-25 09:31:442023-09-06 08:21:27Biotronik partners with EU-funded SIMCor to pioneer heart and blood vessel simulation
A team at the Hebrew University of Jerusalem (HU) is reporting “astounding” results from a trial to check the efficacy of the lipid-lowering drug TriCor (fenofibrate) as a treatment for patients with severe Covid-19.
In earlier research, the team at HU, lead by Professor Yaakov Nahmias, reported that the new coronavirus causes abnormal accumulation of lipids, which are known to initiate severe inflammation in a process called lipotoxicity. Last year the team identified the lipid-lowering drug TriCor (fenofibrate) as an effective antiviral, showing it both reduced lung cell damage and blocked virus replication in the laboratory. These results have since been confirmed by several international research teams. An observational study carried out in multiple clinical centres in Israel was reported last October to support the original findings. The team then launched an interventional clinical study to treat severe Covid-19 patients at Israel’s Barzilai Medical Center with support from Abbott Laboratories.
Now, the HU team is reporting promising results from this trial – an investigator-initiated interventional open-label clinical study led by Nahmias and coordinated by Prof. Shlomo Maayan, Head of Infectious Disease Unit at Barzilai. In this single-arm, open-label study, 15 severe-hospitalized Covid-19 patients with pneumonia requiring oxygen support were treated. In addition to standard of care, the patients were given 145 mg/day of TriCor (fenofibrate) for 10 days and continuously monitored for disease progression and outcomes.
The findings were posted 12 August on Research Square and are currently under peer-review.
“The results were astounding,” said Nahmias. “Progressive inflammation markers, that are the hallmark of deteriorative Covid-19, dropped within 48 hours of treatment. Moreover, 14 of the 15 severe patients didn’t require oxygen support within a week of treatment, while historical records show that the vast majority severe patients treated with the standard of care require lengthy respiratory support,” he added.
These results are promising as TriCor (fenofibrate) was approved by the FDA in 1975 for long-term use and has a strong safety record.
“There are no silver bullets,” stressed Nahmias, “but fenofibrate is far safer than other drugs proposed to date, and its mechanism of action makes is less likely to be variant-specific.”
“All patients were discharged within less than a week after the treatment began and were discharged to complete the 10-day treatment at home, with no drug-related adverse events reported,” noted Maayan. “Further, fewer patients reported Covid-19 side effects during their 4-week follow-up appointment,” he added.
The investigators stressed that while the results were extremely promising, only randomized placebo-controlled studies can serve as basis for clinical decisions.
“We entered the second phase of the study and are actively recruiting patients”, explained Nahmias, noting that two Phase 3 studies are already being conducted in running South America, the United States (NCT04517396) and Israel (NCT04661930).
https://interhospi.com/wp-content/uploads/sites/3/2021/08/covid_patient.jpg12951417panglobalhttps://interhospi.com/wp-content/uploads/sites/3/2020/06/Component-6-–-1.pngpanglobal2021-08-24 16:53:202021-08-24 16:53:20Fenofibrate dramatically shortens treatment time for severe Covid-19 patients – new clinical trials show
The World Health Organization (WHO) recently called on countries to prioritise recognition, rehabilitation and research for the consequences of Covid-19, and the collection of standardised data on Long Covid. They proposed the term “Post Covid-19 Condition” should be used for people living with Long Covid.
A significant portion of people diagnosed with Covid-19 subsequently experience lasting symptoms including fatigue, breathlessness and neurological complications months after the acute infection. However, the evidence for this condition is limited and based on small patient cohorts with short-term follow-up.
Core outcome set
There is an urgent need for the development of a core outcome set (COS) to optimise and standardise clinical data collection and reporting across studies (especially clinical trials) and clinical practice for this condition. With this in mind, clinical research communities and people living with Post Covid-19 Condition have come together to respond to this emerging global healthcare crisis.
An international group of experts in COS development and Post Covid-19 Condition research and clinical practice have developed a programme of research together with WHO, ISARIC (International Severe Acute Respiratory and emerging Infection Consortium), and patient partners to develop a Post Covid-19 Condition COS.
People living with Post-Covid-19 Condition
This project, Post-Covid Condition Core Outcomes, will start by surveying people living with Post-Covid-19 Condition, assess what outcomes matter and build a plan in two phases. The first phase will focus on what outcomes should be measured and the second phase will focus on how to measure these outcomes.
Researchers aim to complete the first phase (what outcomes to measure) in the summer of 2021 and the second phase (how to measure these outcomes) in 2022.
This project follows the COMET (Core Outcome Measures in Effectiveness Trials) Initiative’s standards and has been registered on COMET’s COS registry.
This plan is being globally publicised in its early stages so that research and patient communities are aware, thereby potentially avoiding any unnecessary duplication of work, and to let researchers planning studies, especially clinical trials, and clinicians know the anticipated time frame of these recommendations.
https://interhospi.com/wp-content/uploads/sites/3/2021/08/headache_web.jpg8501134panglobalhttps://interhospi.com/wp-content/uploads/sites/3/2020/06/Component-6-–-1.pngpanglobal2021-08-19 12:52:112021-08-19 12:52:11Researchers start new investigation into Long Covid core outcome set
Fujifilm Irvine Scientific, a specialist in the development and manufacture of cell culture media and assisted reproductive technologies (ART), will become the sole worldwide distributor of Life Whisperer, the fertility arm of Presagen, a leader in Artificial Intelligence (AI) healthcare. Life Whisperer is a web-based software product that uses image-based analysis and AI to assist embryologists in the determination of embryo viability.
While many factors affect the success rate of in vitro fertilization (IVF), the conventional method of determining embryo viability by optical microscopy can be subjective, and critical morphological features that indicate embryo viability may be missed. The Life Whisperer software can aid this process by analysing high-resolution digital camera images taken of Day 5 embryos to assist in identifying embryo morphological features that correlate with uterine implantation potential. The AI algorithm produces a confidence score that objectively indicates an embryo’s implantation potential to produce an objective and standardized embryo viability score, thereby aiding embryologists in their effort to select embryos based on their likelihood of leading to a successful pregnancy.
“We view Presagen’s emerging suite of AI-enabled fertility workflow tools as a strong complement to our portfolio of ART product offerings and aligned with Fujifilm’s broader commitment to AI,” said Tim Mullane, president and chief operating officer, Fujifilm Irvine Scientific.
Steven Geimer, executive director of the Medical Business Unit, Fujifilm Irvine Scientific, commented: “We believe that AI-based ART technology can significantly impact the embryo selection process by providing an objective tool that embryologists can utilize as part of their process to help in the endeavour to increase a patient’s pregnancy potential.”
Presagen developed and implemented a healthcare information network that enables IVF clinics to access the AI tools through the secure and real-time transfer of clinical medical data. That networking platform underpinned the development of the Life Whisperer embryo viability tools.
Dr. Michelle Perugini, chief executive officer and co-founder, Presagen, said: “Life Whisperer tools were developed in collaboration with IVF clinics across the world. Additional fertility tools are under development which will be seamlessly integrated into our current AI platform. This application of AI offers embryologists an objective method of assessing embryo quality to help them increase the chance of a successful pregnancy for their patients. [1]”
The Life Whisperer embryo viability product is expected to be available this summer through Fujifilm Irvine Scientific and its existing distribution channels. The initial offering of the Life Whisperer embryo viability product will be authorized for sale in a number of countries across Europe and Asia Pacific. Additional countries are expected to be added as authorization for use by their respective regulatory agencies is received. It is not for sale in the USA. For more information, visit: irvinesci.com/lifewhisperer
Reference
VerMilyea M, Hall JMM, Diakiw SM, et al. Development of an artificial intelligence-based assessment model for prediction of embryo viability using static images captured by optical light microscopy during IVF. Hum Reprod. 2020;35(4):770-784. https://doi.org/10.1093/humrep/deaa013
https://interhospi.com/wp-content/uploads/sites/3/2021/08/Human_embryo_web.jpg720722panglobalhttps://interhospi.com/wp-content/uploads/sites/3/2020/06/Component-6-–-1.pngpanglobal2021-08-11 08:15:122021-08-11 08:15:12Fujifilm Irvine Scientific becomes sole worldwide distributor of Life Whisperer
Hologic, a global leader in women’s health, has completed its acquisition of Mobidiag Oy, an innovator in near-patient, acute care molecular diagnostic testing, for an enterprise value of approximately US$808 million.
“Closing the acquisition of Mobidiag enables us to become a broader, more diversified global diagnostics leader,” said Jan Verstreken, group president, international at Hologic. “Together, we can accelerate development and adoption of Mobidiag’s innovative products globally and drive Hologic’s growth.”
Mobidiag provides near-patient, molecular diagnostic instruments and tests for acute care conditions including gastrointestinal and respiratory infections, antimicrobial resistance management, and healthcare associated infections. Its Amplidiag and Novodiag testing platforms deliver results in 50 minutes to two hours. The Novodiag platform combines real-time PCR and microarray capabilities to provide high-level multiplexing. Multiplexing enables multiple pathogens to be identified in a single sample, streamlining workflows for laboratories and providing rapid results to physicians.
A small study has found that no Covid-19 mRNA vaccine is present in human breastmilk following vaccination. The study by University of California San Francisco researchers provides early evidence that the vaccine mRNA is not transferred to the infant via breastmilk.
The study analysed the breastmilk of seven women after they received the Pfizer and Moderna mRNA vaccines and found no trace of the vaccine. The findings, although from a small sample, offer the first direct data of vaccine safety during breastfeeding and could allay concerns among those who have declined vaccination or discontinued breastfeeding due to concern that vaccination might alter human milk. The paper appears in JAMA Pediatrics.
The World Health Organization recommends people should continue breastfeeding following vaccination for Covid-19.
The Academy of Breastfeeding Medicine has said there is little risk of vaccine mRNA entering breast tissue or being transferred to milk, which theoretically could affect infant immunity.
“The results strengthen current recommendations that the mRNA vaccines are safe in lactation, and that lactating individuals who receive the Covid vaccine should not stop breastfeeding,” said corresponding author Stephanie L. Gaw, MD, PhD, assistant professor of Maternal-Fetal Medicine at UCSF.
The study was conducted from December 2020 to February 2021. The mothers’ mean age was 37.8 years and their children ranged in age from one month to three years. Milk samples were collected prior to vaccination and at various times up to 48 hours after vaccination.
Researchers found that none of the samples showed detectable levels of vaccine mRNA in any component of the milk.
The authors noted that the study was limited by the small sample size and said that further clinical data from larger populations was needed to better estimate the effect of the vaccines on lactation outcomes.
Reference
Golan Y, Prahl M, Cassidy A, et al. Evaluation of Messenger RNA From Covid-19 BTN162b2 and mRNA-1273 Vaccines in Human Milk. JAMA Pediatr. Published online July 06, 2021. https://doi.org/10.1001/jamapediatrics.2021.1929
https://interhospi.com/wp-content/uploads/sites/3/2021/07/baby.jpg1079727panglobalhttps://interhospi.com/wp-content/uploads/sites/3/2020/06/Component-6-–-1.pngpanglobal2021-07-19 13:25:082021-07-19 13:25:08Study finds no Covid-19 mRNA vaccine in breast milk
We may ask you to place cookies on your device. We use cookies to let us know when you visit our websites, how you interact with us, to enrich your user experience and to customise your relationship with our website.
Click on the different sections for more information. You can also change some of your preferences. Please note that blocking some types of cookies may affect your experience on our websites and the services we can provide.
Essential Website Cookies
These cookies are strictly necessary to provide you with services available through our website and to use some of its features.
Because these cookies are strictly necessary to provide the website, refusing them will affect the functioning of our site. You can always block or delete cookies by changing your browser settings and block all cookies on this website forcibly. But this will always ask you to accept/refuse cookies when you visit our site again.
We fully respect if you want to refuse cookies, but to avoid asking you each time again to kindly allow us to store a cookie for that purpose. You are always free to unsubscribe or other cookies to get a better experience. If you refuse cookies, we will delete all cookies set in our domain.
We provide you with a list of cookies stored on your computer in our domain, so that you can check what we have stored. For security reasons, we cannot display or modify cookies from other domains. You can check these in your browser's security settings.
.
Google Analytics Cookies
These cookies collect information that is used in aggregate form to help us understand how our website is used or how effective our marketing campaigns are, or to help us customise our website and application for you to improve your experience.
If you do not want us to track your visit to our site, you can disable this in your browser here:
.
Other external services
We also use various external services such as Google Webfonts, Google Maps and external video providers. Since these providers may collect personal data such as your IP address, you can block them here. Please note that this may significantly reduce the functionality and appearance of our site. Changes will only be effective once you reload the page
Google Webfont Settings:
Google Maps Settings:
Google reCaptcha settings:
Vimeo and Youtube videos embedding:
.
Privacy Beleid
U kunt meer lezen over onze cookies en privacy-instellingen op onze Privacybeleid-pagina.