
Prins Hendrikstraat 1
5611HH Eindhoven
The Netherlands
info@interhospi.com
PanGlobal Media IS not responsible for any error or omission that might occur in the electronic display of product or company data.


Neonatal intensive care units can be noisy places which can disturb the sleep patterns of the youngest patients in the hospitals and have a negative effect on their health. In an effort to ameliorate this, some NICUs have set quiet times to limit exposure to noise. However, little was known about the effects of the ‘quiet time’ on infant health and it is only now according to a recent study in The Journal of the Acoustical Society of America that researchers have demonstrated its beneficial effect. The study, one of the first in this field, examined the effects of quiet time implementation in multiple NICUs on infants up to 18 months after implementation. They analysed how each NICU’s soundscape changed throughout the day and how this affected infant heart rates. They found that certain stressful pitches were actually quieter in respect to their effect on infant heart rates and that very loud sounds occurred less frequently with the result that quiet time throughout the day was longer. The results provide a sense of which features of quiet time policies have the largest impact on infants in NICUs and they recommend using quiet time protocols to help NICU patients in addition to implementing architectural noise reduction strategies in NICUs.
In a separate, but related study published in Sleep last year, researchers showed that preterm newborns sleep better in NICUs while hearing their mother’s voice. The study explored the possibility that infants’ exposure to their mother’s voice in the NICU could modulate the impact of noise in the NICU. The results indicate that newborns in a NICU were less likely to be awakened by noises when a recording of their mother’s voice was playing. The study also found that newborns born at or after 35 weeks’ gestation show sleep-wake patterns that appear to respond increasingly with age to recorded maternal voice exposure. Similar associations were not found for infants born before 35 weeks’ gestation. It appears that exposure to a mother’s voice recording may insulate NICU patients from some of the impact of unavoidable noise by reducing the likelihood of wakefulness during the highest peak noise levels. Because of this, the researchers suggest that for infants who are ill or born prematurely and may require extended care in a NICU during a time of critical brain development, interventions designed to improve sleep may need to be tailored according to gestational age. As such, the impact of playing a recording of a mother’s voice, reading a story for example, may have a more significant impact for newborns who are near term gestation than for more premature infants.

The ICU (intensive care unit) is easily one of a hospital’s highest value resources. A scarcity of intensive care beds means patients require prioritization when demand exceeds supply. As a result, there are frequent delays in admission to an ICU. Though it is accepted that such delays adversely impact patient outcomes, there has been little data on the relationship between bed availability in an ICU and processes of care for patients who develop sudden clinical deterioration – especially in the context of an emergency department (ED). Recently, studies seeking to address this gap have provided renewed momentum to such discussions. They have also dovetailed with other efforts, such as specialist training in critical care for emergency medicine students and residents. However, the area generating maximum interest is a dedicated ICU within an emergency department.
Balancing needs, finding beds
Critically ill patients are commonplace in emergency medicine. They require aggressive and timely care, but emergency medicine clinicians have to balance their needs with those of other patients in their facility. In addition, due to constraints in beds in the ICU, increasing numbers of critically ill patients require to be boarded for prolonged periods of time in the ED. Adding to this problem is a shortage of beds in EDs too.
One of the most vexed questions is whether ED physicians consider bed availability in an ICU as part of their triage decisions, thereby impacting, in a potentially profound manner, on patient outcomes and resource utilization in both the ED and ICU. In effect, does a high availability of ICU beds lead to a bias in admission of patients who are either too well or too ill to benefit ? On the other side, does a low availability then lead to denying admission to ED patients, who would otherwise have been accepted to the ICU?
ED-ICU interface demands attention
In 2013, a study by the George Washington University School of Public Health and Health Sciences in Washington, DC, found that the volume of ICU admissions from EDs in the US had increased sharply, by almost 50 percent, in the period 2001-2009.1 During this period, another study found that the number of ICU beds across the country had increased only 15%, from 67,579 to 77,809.2
In other words, it is clear that ICU admissions from EDs have been increasing at a faster rate than ED visits. The George Washington University study found that though lengths of mean ED and hospital stays had not changed significantly, the mean ICU admission spends over 5 hours in the ED prior to transfer to an ICU bed. As a result, its authors concluded, there was a need for more emphasis on the ED-ICU interface and for critical care delivered in the ED.
Training emergency physicians in the ICU
The roots of this complex combination of challenges go back several decades. One good example is a time-based study, published in 1993 in the peer-reviewed journal ‘Critical Care Medicine’.3 The authors, from Houston, Texas-based Methodist Hospital’s Department of Emergency Services, noted that not only did critically ill patients “constitute an important proportion of emergency department practice”, but also needed treatment in the ED “for significant periods of time.” One of the solutions they proposed was for emergency medicine practitioners to “receive training in the continuing management of critically ill patients.”
The above approach was also witnessed in Europe. In Belgium, for example, an official paper from 1995, titled ‘How to become an intensivist’, proposes that a candidate with an “agreement in Emergency medicine has to make another year of ICU formation.”4
Pathways remained unclear
In subsequent years, there was significant growth in emergency medicine residents pursuing critical care fellowship training, and a reconsideration of the role played by the ED in caring for the critically ill. Nevertheless, there still was a lack of clarity in ways to acquire advanced training in critical care for emergency medicine residents.
In December 2002, an article in ‘Current Opinion in Critical Care’ complained that although ED care for critically ill patients was shown to significantly impact mortality, “formal critical care training for emergency physicians” was still “limited.”5
Less than three years later, another peer-reviewed journal, ‘Annals of Emergency Medicine’, noted that in spite of growing demand for critical care services, most critical care medicine fellowships did not accept emergency medicine residents, “and those who do successfully complete a fellowship do not have access to a US certification examination in critical care medicine.”6 The authors proposed “expansion of the J-1 visa waiver program for foreign medical graduates,” but said the only sensible long-term approach was to strengthen the relationship between emergency medicine and critical care medicine.
Critical care medicine as emergency medicine sub-specialty
In the US, the Accreditation Council for Graduate Medical Education (ACGME) approved critical care medicine as a sub-specialty for emergency medicine physicians in 2011. The following year, the surgical critical care fellowship pathway was approved for emergency physicians interested in becoming board-eligible intensivists.
Currently, the most common training pathways are via combinations of critical care medicine with internal medicine and anaesthesiology, and alongside surgical critical care and neurocritical care. Career pathways for physicians trained in emergency and critical care medicine are also evolving, with options in both community and academic settings.
The role of professional societies
Leading professional societies in emergency medicine and critical care have set up focused sections on the interface between the two areas to stimulate interest as well as provide support to medical students and residents.
Examples from the US include the Emergency Medicine Residents’ Association (EMRA), whose Critical Care Division maintains a comprehensive database of training opportunities across the country,7 and regularly publishes alerts on key developments in critical care. Another interesting initiative is the Coalition for Critical Care Medicine in the Emergency Department (C3MED), which was set up in 2003 and hosts an active email discussion forum.8
Similar efforts have been undertaken by the American College of Emergency Physicians (ACEP),9 the Society of Critical Care Medicine (SCCM),10 the American Association of Emergency Medicine11 and the Society for Academic Emergency Medicine (SAEM).12
In Europe, one of the best-known initiatives to harmonize convergence of the ED and the ICU is ISICEM, the International Symposium on Intensive Care and Emergency Medicine. This non-profit organization, headquartered in Brussels, was set up in 1980. It currently runs a series of eight annual events, covering different aspects of intensive care and emergency medicine. Over the years, participation has grown from about 200 to over 6,000 from more than 100 countries.
Impact of ED on ICU: US and European studies
There have also been concerted efforts to assess the impact of emergency department volume and boarding times on ICU admission and patient outcomes. Two recent studies have catalysed considerable new attention in the topic.
The first is a retrospective cohort study on critically-ill ED patients for whom a consult for medical ICU admission had been requested over a 21-month period. It was published in ‘Critical Care Medicine’ last year by a US-based team from the Icahn School of Medicine at Mount Sinai, New York, and titled ‘Effect of Emergency Department and ICU Occupancy on Admission Decisions and Outcomes for Critically Ill Patients’.
The authors conclude that ICU admission decisions for critically ill ED patients were affected by ICU bed availability. However, higher ED volume and other ICU occupancy did not play a role. They also found that prolonged ED boarding times were associated with worse patient outcomes, suggesting a need for improved throughput and targeted care for patients awaiting ICU admission.
In August 2019, ‘Critical Care Medicine’ published findings online from another study on this topic, this one by a Dutch team from six University Medical Centres at Amsterdam, Groningen, Leiden, Nijmegen, Rotterdam and Utrecht, along with the country’s National Intensive Care Evaluation (NICE) foundation.13 The retrospective observational cohort study conducted a registry analysis of 14,788 patients from the six hospitals, and found an association between emergency department to ICU time greater than 2.4 hours and increased hospital mortality after ICU admission
Ad-hoc and hybrid models
At present, there are two approaches to the challenge of intensive care in the ED. The more common is to have an emergency physician intensivist working standard ED shifts, and lending expertise on an ad-hoc basis to critically ill patients. A recent development is a ‘hybrid’ model. This earmarks a dedicated area of the emergency department for ramping up care to critically ill patients, with a dedicated physician providing intensive care only to such patients, typically for periods longer than an hour.
Supporters of the hybrid model state that it is easier and less expensive to establish with extra costs involving only the dedicated ED-ICU physician.
The ED-ICU
One of the most watched developments in recent years in care for critically ill patients in an ED is the development of ED-ICUs (emergency department intensive care units).
Two such facilities in the US, Stony Brook Resuscitation and Acute Critical Care Unit (RACC) in New York and Emergency Critical Care Center (EC3) in Michigan are considered as being both ED-ICU pioneers and best-of-class references for the concept.
EC3 is considered to be among the world’s most advanced emergency critical care centres. It was opened in February 2015 and has five resuscitation trauma bays and nine patient rooms, located adjacent to the main adult emergency department.
Due to this reputation, the case for ED-ICUs was strengthened after a recent study by EC3 found convincing improvements in survival as well as reduced inpatient ICU admissions.14 In effect, an ED-ICU can improve care and survival rates for the entire emergency department population.15
The EC3 study covered 350,000 ED patient encounters, and found that implementation of an ED-based ICU was associated with significant reductions in risk-adjusted 30-day mortality among patients, from 2.13 to 1.83 percent. The median time to ICU-level care for critically ill patients decreased from 5.3 hours to 3.4 hours, while the hospital ICU admission rate from the ED dropped from 3.2 percent to 2.8 percent.
References
1.https://www.sciencedaily.com/releases/2013/05/130514212946.htm2.https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4351597/3.https://www.ncbi.nlm.nih.gov/pubmed/8319477/4.http://www.siz.be/education/training-in-critical-care/5.https://www.ncbi.nlm.nih.gov/pubmed/124545496.https://pdfs.semanticscholar.org/4f1b/5cea333174e599784e6a2d80c9b55b868b2e.pdf7.https://www.emra.org/fellowships/critical-care-fellowships/8.c3med@yahoogroups.com9.https://www.acep.org/criticalcaresection/10.http://www.sccm.org/Member-Center/Sections/Pages/Emergency-Medicine.aspx11.http://www.aaem.org/membership/critical-care-section12.https://community.saem.org/communities/community-home?CommunityKey=5dc206d8-d248-4f71-aecd-e0490cdc3ba913.https://insights.ovid.com/pubmed?pmid=3139332114.https://jamanetwork.com/journals/jamanetworkopen/fullarticle/273862515.https://medicalxpress.com/news/2019-07-department-based-intensive-patient-survival.html

The term “artificial intelligence”, defined in the Oxford Dictionary as “the capacity of a machine to simulate or surpass intelligent human behaviour”, was first used in the 1950s, but the idea that the human brain, or at least parts of it, could somehow be ‘copied’ or ‘imitated’ using a series of mechanical networks has been part of myth and literature for centuries, as far back as, for example, the automatons of Hephaestus and Daedalus.
by Prof Jean-Louis Vincent
Artificial intelligence is an umbrella term that covers multiple tools and technologies. In recent years, huge advances in machine learning algorithms, neural networks, deep learning, facial recognition, computing power and statistical techniques have increased the potential applications of artificial intelligence across multiple aspects of everyday life. In terms of medicine, artificial intelligence is already beginning to find a place in disease prediction and diagnosis, clinical decision support and therapeutic guidance, prognostication, and remote follow-up and monitoring.
So, what do these new developments mean for the medical profession – is this ever advancing technology going to decrease the need for doctors? To some extent, the answer is of course yes, perhaps particularly in the field of diagnostics. Using machine learning, computerized systems are able to study and develop pattern recognition from millions of test results over a very short period of time, whereas a doctor can only see and process a limited number of events throughout a whole professional career. The vast amounts of data becoming available as increasing numbers of patients have electronic health records and are managed with electronic monitoring systems are providing the input needed for artificial intelligence to develop, while also reducing the administrative load on doctors and other healthcare staff, a common source of complaint. Machine-based interpretation of visual data is now more accurate, effective, and rapid than the human eye and associated with less risk of error. Interpretation of X-rays and other medical images will become increasingly automated, reducing the need for radiologists to perform this role. Similarly, electrocardiograms are already read automatically; many of the reports are still validated by a cardiologist, but is this really necessary? In ophthalmology, examination of the fundus for many diagnoses, including diabetic retinopathy and macular degeneration, can be performed more accurately by computerized algorithms than by most experienced ophthalmologists. Application of deep learning to a database of eye CT-scans at a London hospital has enabled more than 50 ocular diseases to be recognized by the system. Non-image-based diagnosis is also possible. A pilot system developed in California that applied machine learning to electronic health record data has been used to diagnose common pediatric problems and shown to perform better than junior doctors.
Although artificial intelligence may therefore indeed reduce the need for doctors in some areas, this is not necessarily a bad thing; it should not be seen as the enemy, but rather as a means of improving medical practice and patient care. More rapid, accurate diagnosis can only be positive. Another important example of how artificial intelligence can be beneficial is in predictive medicine. Natural language processing of data from electronic medical records was able to more accurately predict postoperative complications in patients undergoing major surgery than were patient safety indicators. Machine learning-based sepsis prediction has been associated with reduced mortality rates. Indeed, early identification of patients with an increased risk of sepsis raises awareness and facilitates early investigation and management by sepsis-trained physicians in a condition where rapid diagnosis and treatment are crucial to maximize chances of survival. More broadly, identification of patients at risk of deterioration on the general floor or after surgery will enable appropriate monitoring systems to be offered to a selection of patients in an environment where it is not feasible, financially or practically, to monitor every hospitalized patient.
Another example is the field of therapeutics. Machine-learning can identity the most effective therapeutic algorithms for individual patients, with the most appropriate evaluation and follow-up. These algorithms are being incorporated into closed-loop systems enabling appropriate treatments to be administered and doses adjusted in real-time for individual patients according to continual personal data provision. Just some of many examples include implantable cardioversion defibrillators, diabetes management with implantable glucose monitors and insulin pumps, and use of vasopressors to prevent hypotension during surgery.
Artificial intelligence can thus be used to provide continually adjusted, up-to-date, patient-relevant information on the best therapeutic options for a specific patient much more rapidly and accurately than doctors can. Doctors can currently assimilate only a small portion of the information available on which to base such decisions. By configuring the huge amounts of patient data now available into predictive models, machine learning can provide physicians with recommendations regarding the optimum treatment schedule for a specific patient with a specific condition(s). Doctors are still needed to interpret the recommendation, explain them to the patient and their family, and initiate the chosen treatment course. Using artificial intelligence, doctors will be more enabled to select the optimum treatment regimens for individual patients, rather than the one-treatment-fits-all packages that are still used for many conditions today. Moreover, doctors will have greater access to accurate statistics to inform discussions with patients and their families, both about the likely outcomes from different treatment options, but also about likely prognosis if treatment is refused or withdrawn. The role of doctors in this situation will increasingly be one of advisor as patients become ever more involved in their own healthcare decisions.
Artificial intelligence is going to continue to invade every aspect of daily life, including medicine, and needs to be carefully developed and validated. Although currently very much associated with rich economies of the developed world, artificial intelligence could play a large role in improving healthcare in countries where qualified doctors are less widely available. These new technologies could therefore help to decrease inequalities in the health sector. Even in low income countries, the combination of artificial intelligence with telemedicine can help increase access to high quality medicine. Wherever it is employed, it will not entirely replace doctors but rather make them more efficient, provide more time for one-to-one patient contact and help provide care best adapted to individual patients, with reduced errors. People often raise the question of associated costs. But costs may not be very high, especially as the technology becomes more widely used. Indeed, artificial intelligence may even help reduce global healthcare costs by increasing efficiency.
Doctors should not fear this technology, but learn to accept and embrace it, determining and directing how it can best be incorporated into medical practice to improve patient care.
The author
Jean-Louis Vincent, MD, PhD
Dept of Intensive Care, Erasme Hospital, Université libre de Bruxelles, Brussels, Belgium
Suggested reading:
Darcy AM, Louie AK, Roberts LW. Machine learning and the profession of medicine. JAMA 2016;315:551-2.
De Fauw J, Ledsam JR, Romera-Paredes B, et al. Clinically applicable deep learning for diagnosis and referral in retinal disease. Nat Med 2018;24:1342-1350.
Joosten A, Alexander B, Duranteau J, et al. Feasibility of closed-loop titration of norepinephrine infusion in patients undergoing moderate- and high-risk surgery. Br J Anaesth 2019 Jun 26. doi: 10.1016/j.bja.2019.04.064129
Kilbride MK, Joffe S. The new age of patient autonomy implications for the patient-physician relationship. JAMA 2018;320:1973-1974
Liang H, Tsui BY, Ni H, et al. Evaluation and accurate diagnoses of pediatric diseases using artificial intelligence. Nat Med 2019;25:433-438.
McCoy A, Das R. Reducing patient mortality, length of stay and readmissions through machine learning-based sepsis prediction in the emergency department, intensive care unit and hospital floor units. BMJ Open Qual 2017;6:e000158
Murff HJ, FitzHenry F, Matheny ME, et al. Automated identification of postoperative complications within an electronic medical record using natural language processing. JAMA 2011;306:848–855.
Topol EJ. High-performance medicine: the convergence of human and artificial intelligence. Nat Med 2019;25:44-56
Vincent JL, Creteur J. Big data are here to stay! Anaesth Crit Care Pain Med 2019;38:339-340.
Vincent JL, Einav S, Pearse R, et al. Improving detection of patient deterioration in the general hospital ward environment. Eur J Anaesthesiol 2018;35:325–333.
Sepsis is a potentially fatal condition after the immune system over-reacts to an infection, leading to shock and organ failure. It is most frequently provoked by commonplace bacteria. Globally, over 30 million people develop sepsis each year. Some 6 million die as a result. Although there has been progress in controlling deaths from sepsis in recent decades, the challenge is still a major one. Indeed, in industrialized countries, the incidence of sepsis is higher than that of new cases of cancer.
Unpredictable and terrifying
Sepsis is frequently encountered in a hospital setting. It is also a leading cause for hospital readmission. In the US, studies estimate that one of 3 people who die in hospital have sepsis.
One of the biggest challenges for clinicians is that sepsis occurs unpredictably and progresses at terrifying speed. This makes timely diagnosis a tough call.
Definitions of sepsis have also tended to vary. In 2018, a working group of 19 specialists, convened by the Society of Critical Care Medicine in the US and the European Society of Intensive Care Medicine (ESICM), updated the clinical definitions and criteria for sepsis and septic shock. The taskforce recommended defining sepsis as “life- threatening organ dysfunction caused by an inappropriate host response to infection.” It also concluded that the term ‘ severe sepsis ‘ was redundant.
Rory’s Regulations
Nevertheless, there has been some progress in recent years in understanding sepsis and standardizing approaches to diagnose, manage and treat the condition.
In 2012, Rory Staunton, a healthy 12-year-old from New York, died due to the fact that his sepsis was not diagnosed. In the wake of this, the government of New York State mandated all hospitals to comply with protocols to improve the early diagnosis and treatment of sepsis and septic shock, and made it compulsory for reporting all sepsis cases to the Department of Health.
The New York Sepsis Initiative, which the media called Rory’s Regulations after the young victim, essentially consist of two treatment bundles.
The first is a 3-hour bundle, and is indicated for patients with severe sepsis and needs to be activated within three hours of a patient’s arrival at hospital. It includes blood culturing to determine choice of antibiotics, starting antibiotic treatment and assessing blood lactate levels – an important marker for sepsis.
The second, 6-hour bundle, is earmarked for patients with septic shock and needs to be carried out within six hours of their arrival at hospital. It includes administration of intravenous fluid, vasopressors to contract blood vessels and a follow-up check on lactate levels.
Assessing the New York Sepsis Initiative
The New York Sepsis Initiative was assessed earlier this year by a team from Warren Alpert Medical School at Brown University. They studied data from 91,357 patients, treated over a period of 27 months at 183 hospitals.
The findings were encouraging. The two sepsis bundles were used in 81.3 percent of patients. After implementation of the protocols, compliance steadily increased across hospitals in the State. The study’s most important finding, however, was that patients administered the bundles saw a reduction in mortality risk over 4 percentage points, at 24.4 percent. The mortality risk in those who did not receive the bundles was 28.8 percent. In addition, hospitals complying with the protocols saw a significant reduction in average length of stay.
Limits to fighting sepsis
While the New York State initiative provides strong evidence of the potential for standardizing sepsis-fighting measures, another study this year shows there may be limits to its scope. The study, by researchers from Brigham and Women’s Hospital in Massachusetts, was published in March by ‘JAMA Network Open’. It sought to investigate the precise role of sepsis in hospital deaths and estimate how many were preventable.
The researchers studied records of 568 people from six acute care hospitals for the years 2014 and 2015, who had died in the hospital or after discharge to hospice care. Using a 6-point Likert scale, ranging from “definitely preventable” to “definitely not preventable,” they concluded that some 90 percent of deaths were not preventable in a hospital setting. On the other side, 1 in 8 sepsis-related deaths were deemed “potentially preventable with better hospital-based care.”
The key reason for such a prognosis was that most sepsis fatalities occur in medically complex, older patients with severe co-morbidities, including chronic conditions such as cancer, heart and lung disease. In the few cases of death due to sub-optimal care, the most common causes included late antibiotic administration.
The lead author of the study, Dr. Chanu Rhee, called for more “innovation in the prevention of underlying conditions” to reduce sepsis mortality by a significant margin.
Long term decline in sepsis death rates
Although the challenge of sepsis remains serious, there has been significant progress over recent decades. In October 2018, the annual meeting of ESICM (the European Society of Intensive Care Medicine) was presented with an analysis of 30-year trends in sepsis deaths. Using World Health Organization figures, researchers from Harvard Medical School and Imperial College London (ICL) found that the average death rate from sepsis in Europe, North America and Australasia fell from 36.2 per 100,000 men in 1985 to 27.1 in 2015, and for women, from 23.2 per 100,000 women to 19.6.
Countries which managed to reduce death rates most significantly were Finland, Iceland and Ireland, while increased rates were noted in both Denmark and Lithuania.
Prospects for managing and treating sepsis in future years is likely to improve due to several new weapons, ranging from targeted drug development to artificial intelligence. Growing interest in this field is indicated by more than 200 sepsis biomarkers approved by the US Food and Drug Administration (FDA), among them interleukins, C-reactive protein and procalcitonin.
MIT’s IL-6 sensor system
It is known that interleukin-6 (IL-6), a protein produced in response to inflammation, begins to increase a few hours prior to other sepsis symptoms. IL-6 levels have not been strong enough to be detected by traditional tests. However, new sensor technologies appear to offer promise.
Researchers at the Massachussets Institute of Technology (MIT) have developed a small microfluidic sensor which can reportedly detect sepsis in a small blood sample (such as that obtained from a finger prick) within 25 minutes. The system uses antibody-laced magnetic microbeads in one fluid channel, which mixes with the blood sample and identifies the IL-6 biomarker. Meanwhile, another channel attaches the biomarked beads to an electrode. When a current is run through the electrode, a signal is produced each time an IL-6 bead passes through.
The magnetic detection system is far less expensive than the high-end optics required by conventional assays, and requires far less blood. The MIT researchers state that they will eventually be able to detect minute increases in IL-6 during the test itself. They are now continuing work on researching other proteins which act as early markers for sepsis detection and would reinforce diagnostic accuracy.
Early warning sepsis indicator
A new hematological biomarker, introduced in 2018 by Beckman Coulter as the Early Sepsis Indicator, is reported as part of a routine complete blood count (CBC) and measures morphological changes in monocytes, cells which play a role in the dysregulated immune response to sepsis. A positive result alerts clinicians to a higher probability of sepsis at an early stage
Thermography tools
Another novel diagnostic technique is based on the fact that abnormal body temperature patterns accompany the earliest stages of sepsis. University of Missouri researchers have proposed using infrared thermography to measure the difference between body extremities and a patient’s core temperature. The team have developed an automatic real-time system which calculates this, based on a frontal and lateral infrared thermogram of the face. Writing in a recent edition of the ‘International Journal of Data Mining and Bioinformatics’, they state the system works successfully, irrespective of the angle of the head relative to the imager and differences in backgrounds.
Targeting enzymes
Other efforts involve new drugs. One priority consists of signalling pathways which control immune cell behaviour during sepsis. So far, most research on inflammation has focused on kinases, the enzymes which transfer phosphate groups to specific substrates.
In August 2019, researchers from the University of California San Diego (UCSD) School of Medicine discovered a wholly new target area – the enzymes which remove them. In particular, they focused on PHLPP1, an enzyme which impacts upon inflammation by removing phosphates from the transcription factor known as STAT1, which controls inflammatory genes.
Using a mouse model, the researchers administered live E. coli bacteria and lipopolysaccharide (LPS), to both PHLPP1-deficient and normal mice. They found that the former fared far better, with half surviving infection-induced sepsis after 5 days – compared to zero for normal mice. The UCSD researchers believe that inhibiting PHLPP1 might form the basis for new sepsis treatments in humans, offering the means to control the dangerous inflammation of sepsis while maintaining the critical bactericidal properties of white blood cells.
Non-antibiotic drugs against sepsis
Researchers at the Royal College of Surgeons in Ireland (RCSI) have tested a compound called cilengitide (brandname InnovoSep) in a preclinical trial. A key feature of InnovoSep is that it is not an antibiotic, and does not face the limitations associated with the latter – namely, the need for rapid identification of causative bacteria and growing resistance to antibiotics.
Cilengitide is an antagonist of alpha-v beta-3, the key endothelial cell integrin which mediates the adhesion of cells to the extracellular matrix. In everyday terms, the drug prevents bacteria “from getting into the bloodstream from the site of infection by stabilizing the blood vessels so that they cannot leak bacteria and infect the major organs,” according to Steven Kerrigan of the RCSI.
Artificial intelligence
To some, however, artificial intelligence (AI) is seen as potentially the most exciting frontier in the fight against sepsis. In 2018, the journal ‘Nature Medicine’ featured an AI system developed by scientists at Imperial College London, which proved to be more reliable predicting the best treatment for sepsis, as compared to human doctors. This was after it had ‘learned’ from an analysis of 100,000 patient records and clinical decisions in intensive care units about sepsis over a 15-year period.
Another promising AI system against sepsis has been developed by Sentara Healthcare in the US. Sentara’s sepsis prediction tool is based on identifying at-risk patients by using an algorithm to spot patterns from some 4,500 pieces of data in an electronic record. These focus on metrics such as body temperature, heart rate, blood tests, gender, medical history, etc.. Sentara had previously developed a ‘sepsis sniffer’ which detected when a patient had just begun to have sepsis. The current system goes further, and does not wait until a patient has already developed the disease.

In 1985, two colleagues from American Science and Engineering, Jay Stein and David Ellenbogen, founded Hologic to commercialize a bone scanning system that employed X-ray technology. It would become the world’s first X-ray bone densitometer for evaluating osteoporosis. Over the years, Hologic has acquired complementary companies that have enabled it to become a global player in women’s health and the undisputed market leader in mammography.
International Hospital talked to Pete Valenti, Division President, Breast and Skeletal Health Solutions at Hologic to learn more about the latest developments and strategy of this innovation-driven company.
1. Hologic is most generally associated with mammography and breast disease diagnosis. However, that’s not the whole story. How would you define the current positioning of the company?
Hologic was the first company to bring digital breast tomosynthesis (DBT) to market, forging the path for how mammography exams are approached today, so it comes as no surprise that the company is most generally associated with breast cancer screening. However, as you suggest, screening is only one part of Hologic’s full story.
A global leader in women’s health, Hologic is primarily focused on improving women’s health and well-being through early detection and treatment across four divisions: Breast & Skeletal Health, Diagnostics, Gynecological Surgical Solutions and Cynosure, our medical aesthetics division. Each division is built on a foundation of the exceptional, clinically proven ability of our products to detect, diagnose and treat illnesses and other health conditions earlier and better, while also keeping in mind clinicians’ needs such as workflow efficiency.
2. Recently, Hologic has expanded its breast health product line significantly, could you briefly describe some of these innovative product launches?
We have spent the past several years thoughtfully expanding our breast health portfolio through a commitment to insight-driven innovation and strategic acquisitions that align with our mission. Now we can make a positive impact on breast health at each step of a woman’s journey – from screening to pathology.
The Trident® HD specimen radiography system and the LOCalizer™ wire-free guidance system are two products that launched in 2019 under our new breast surgery franchise.
The Trident HD system is a next-generation solution that delivers enhanced image quality, improved workflow and instant sample verification during breast-conserving surgeries and stereotactic breast biopsies, while the LOCalizer system is designed to enable precision and ease of use for breast surgery guidance. The system’s LOCalizer tag is designed to replace traditional wire-guided methods, helping provide increased comfort and convenience for patients and their healthcare teams.
Both products have received CE Mark in Europe and reflect Hologic’s aim to benefit both patients and clinicians by arming them with accurate, efficient technology.
3. This expanded product portfolio is enabling the company to be active in breast conserving surgery as well as pathology. Do you see these segments as a major growth opportunity?
I absolutely see breast conserving surgery and pathology as growth opportunities for Hologic; and, as touched upon earlier, I believe our expansion into these parts of the breast care continuum is also about making as much of a positive impact as possible for patients and clinicians throughout the entire pathway of care.
4. There have also been some strategic acquisitions lately, for example with the LOCalizer. Is this a scenario that might be repeated in the near future?
At Hologic, we are in a fortunate position where we are able to both innovate healthcare solutions from within and make strategic acquisitions from external sources. As opportunities arise, we are always willing to examine how we can continue to impact patients and clinicians in a positive way through new and consistently high-quality technology.
5. What do you see as the next step for Hologic?
Hologic will continue to work to bring to market crucial healthcare solutions that address both patients’ and clinicians’ needs by taking into consideration all factors, from accuracy and workflow efficiency, to the patient experience and beyond. It is approaching innovation with this holistic view that sets Hologic apart as an industry leader, and by bringing this mindset into new areas of the healthcare continuum like breast conservation surgery, I believe Hologic will make an even greater positive impact on the lives of women across the globe.
I think we’ll also see great evolution in our technology and approaches to risk stratification as we continue to explore how to best leverage the benefits of artificial intelligence to support clinicians and the important work they are doing.
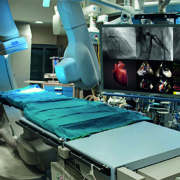
A hospital or healthcare facility can be composed of dozens of departments. A catheterization lab, commonly referred to as cath lab or EP lab, is instrumentally vital to one of the busiest departments, cardiology. Hybrid OR’s are equipped with diagnostic imaging technology to give physicians visual access to chambers and arteries of the heart. In these areas, physicians perform life-saving procedures including coronary artery bypass graft surgery, balloon angioplasty, congenital heart defect closure, stenotic heart valves, and pacemaker implantations.
These acute procedures would not have been practicable without the appropriate technology to facilitate the imaging process. Cath lab operations are dependent on medical displays, as these monitors allow physicians to visualize a patient internally and perform the necessary procedure. In a single medical procedure, up to 4-6 monitors can be utilized at any time for enhanced visibility.
Although many monumental advancements have been made in the efficiency of cath labs, the dependence on X-rays for imaging has persisted through every upgrade. From purchasing analogue or digital modalities to choosing a single or bi-plane system, there are endless customization possibilities. Typically, the rooms are equipped with an image intensifier, C-arm, X-Ray tubes, and several displays.
Advantageously, the digital age ushered in an era of improvements to imaging technology, which emitted less radiation, and displayed visual clarity. The adoption of CRT monitors in the cath lab inherently changed how labs ran.
In the early cath labs, all information was conveyed through film. The X-rays, produced high-doses of radiation and low-quality images, which were printed on 16-mm or 35-mm film. Then, radiologists spent many hours of the day in darkrooms to process images, and ample storage space was wasted holding boxes of film.
With the implementation of picture archiving and communication systems (PACS), the transition from analogue to digital technology was concretized. PACS is an all-in-one program that provides electronic storage, retrieval, distribution, and presentation of radiology images.
In the cath lab, there are typically four to six CRT or LCDs in use. One image is always utilized for monitoring physiological attributes like a patient’s heart rate or blood oxygen level. Following CRT displays was the adaptation of LCD monitors. Many physicians upgraded to these monitors since they are slimmer, more portable, and offer higher resolution images.
“We are witnessing yet another transition in Cath Lab, Hybrid OR monitors as many physicians are upgrading from CCFL HD displays to ultra-high-definition 4K/8MP technology” says Michael Thomas Director of Business Development & Marketing at Ampronix. Many healthcare facilities have upgraded or are currently in the process of upgrading their medical displays to this resolution. These monitors provide a level of visibility previously unknown to physicians. During critical surgeries and procedures, increased clarity and sharper details can mean the difference between saving or losing a life.
These 4K/8MP large medical-grade displays are considered to be the new “gold standard” for surgical applications, allowing multiple screens to be viewed on a single monitor while taking up a minimal amount of space. When a 4K/8MP display is combined with a video manager, it can become customizable with a variety of layout options and editing tools like magnification. The design is easier to use and provides a higher resolution, making its adoption an easy choice as it facilitates precise procedures and minimally invasive surgeries.
Although the advancement of this technology has improved patient care, the transition made could prove to be detrimental and may demand considerable attention. With four to six displays in the cath lab previously, there are preventative measures in place that guarantee a backup option should a monitor burn out. In critical imaging procedures like angioplasty, mere seconds without visibility become crucial moments, and a single display makes cath labs extremely susceptible to all the risks associated.
To solve this issue, some displays are equipped with a secondary back-up monitor that folds out, if needed. However, this is a sacrifice that presents limited visual acuity. When this situation unravels, the entire procedure must be halted and the patient sutured up, as technicians attempt to remedy the problem.
Furthermore, any display failure amounts to an entire cath lab rendered obsolete until a replacement or repair solution is provided. Unfortunately, the turn around time for either of those protocols can take over a week.
THE SOLUTION
Ampronix has been repairing & selling 4K monitor’s sized 56”, 58”, & 60” for Cath Labs, & Hybrid OR’s to hospitals for years.
We are able to sell, service and repair the follwing Cath Lab monitor manufactures:
Philips, GE, Siemens, Shimadzu, Toshiba, Hitachi, Eizo, Barco, Chilin, Optik View
• Savings on costs and reduced downtime
• Most models are in stock and sold at half the OEM price
• Next day delivery by 10am or same day delivery available
• Services include preventive maintenance, replacement of LCD, backlights, reflectors, and power supplies
• Remote adjustments are available
We know how important your Cath Lab is and want to ensure you have Zero Downtime in the event your monitor will need service or replacement.
We offer:
• Nationwide requests received by 2pm PST will receive same or next day delivery
• A readily available response team to assist and answer questions for urgent repairs
• ESD and ASQ certified technicians
• Capable and competent customer service representatives for all your medical
technology questions and concerns

By Callan Emery, Editor
A study published in Nature in September has caught the attention of the media and the interest of
Obs-Gyn specialists. In what is the largest study of the neonatal microbiome (gut bacteria), the researchers provide strong evidence that the way a baby is born impacts significantly on their microbiome.
The study by Lawley T., et al. (doi: 10.1038/s41586-019-1560-1) found that babies born through the vaginal canal carry different microbes from those delivered through caesarean section. Those born through c-section tended to lack strains of gut bacteria found in healthy children and adults. Additionally babies born through c-section showed a high-level of colonization by opportunistic pathogens associated with the hospital environment (including Enterococcus, Enterobacter and Klebsiella species).
Interestingly, the researchers note that it was the mother’s gut bacteria, and not vaginal bacteria, that made up much of the microbiome in the vaginally delivered babies. Previous studies had suggested that vaginal bacteria were swallowed by the baby on its way down the birth canal. This led to what is has been termed ‘vaginal seeding’ whereby babies born by c-section are swabbed with the mothers vaginal fluids in an effort to restore any missing microbes. However, a study by Stinson et al. (doi: 10.3389/fmed.2018.00135) has shown vaginal seeding to be unjustified and potentially unsafe.
Although a lack of exposure to the right microbes in early childhood has been implicated in autoimmune diseases, such as asthma, allergies and diabetes, the exact role of the baby’s gut bacteria is unclear and it isn’t known if these differences at birth will have any effect on later health.
The researchers, who analysed nearly 600 births in the United Kingdom, say the differences in gut bacteria between vaginally born and caesarean delivered babies largely evened out by 1 year old. They note that large follow-up studies are needed to determine if the early differences influence health outcomes.
Discussing her study, Stinson pointed out that microbes thrown out of balance in babies born by c-section are very similar to those thrown off balance in babies born to mothers receiving antibiotics but delivering vaginally. She surmises that routine antibiotic administration given to mothers delivering by c-section could be a cause of the bacterial difference in the neonatal microbiome.
Although this research does pose interesting questions about the potential health outcomes associated with c-section versus vaginal delivery, it should be emphasised that at this point mothers should not be deterred from c-section delivery if it is the right choice for the mother and her baby.
The study is part of larger effort, called the Baby Biome Study, which aims to follow thousands more newborns into childhood.


Prins Hendrikstraat 1
5611HH Eindhoven
The Netherlands
info@interhospi.com
PanGlobal Media IS not responsible for any error or omission that might occur in the electronic display of product or company data.