

Despite significant inherent advantages of liquid chromatography-tandem mass spectrometry (LC-MS/MS) over immunoassay techniques in clinical laboratory applications, its adoption into routine practice has been slower than might have been expected. The barriers to more widespread uptake are a function of issues in the laboratory workflow. This article analyses those issues and discusses how they can be overcome by improved automation and integration with the laboratory information management system, drawing on examples from the North West London Pathology (NWLP) clinical laboratories at Imperial College Healthcare NHS Trust.
by Dr Emma L. Williams
Introduction
Liquid chromatography-tandem mass spectrometry (LC-MS/MS) has seen over two decades of use in specialist clinical laboratories in the UK, offering a number of significant advantages over immunoassay techniques. These advantages include increased specificity, sensitivity and accuracy, as well as the detection of multiple analytes within a single assay. There is no need for an antibody for analyte detection and the method is not susceptible to the antibody-based interferences that plague immunoassays [1]. LC-MS/MS is suitable for multiple sample matrices and avoids the need for radioactive tracers. LC-MS/MS assays also have a wider dynamic measurement range and have improved between-method bias when compared to immunoassays.
LC-MS/MS initially played a role in specialist clinical laboratories in areas such as newborn screening, inborn errors of metabolism, toxicology and in immunosuppressant and therapeutic drug monitoring. More recently LC-MS/MS has established a role in diagnostic endocrinology, with the first appearance of LC/MS-MS for the measurement of vitamin D in the international vitamin D external quality assurance scheme (DEQAS) in 2005. There are now over 150 labs registered in this scheme using LC/MS-MS for the measurement of vitamin D. However, automated immunoassay still dominates and represents 69% of participants registered in the DEQAS scheme. Why has there not been more widespread adoption?
A number of issues have inhibited wider adoption and routine use of LC/MS-MS in the clinical laboratory. First among these is the use of labour-intensive manual workflows, which result in lower throughput, decreased productivity and longer turnaround time. Furthermore, a high level of technical expertise is needed, not only for method development, but also for troubleshooting assay and equipment failures. In addition to the high initial capital costs of purchasing the equipment, ongoing personnel costs are higher because of the need for more technically competent staff. With a clear understanding of where the bottlenecks in the process arise, these barriers can be overcome.
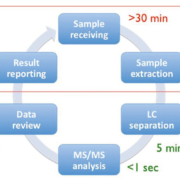
Figure 1 depicts the six main steps of a typical LC/MS-MS workflow, from sample receipt and extraction, separation in the LC, MS/MS analysis, data review and reporting of the results [2]. Of these steps it is the pre- and post-analytical stages that are the most time consuming and therefore if there is a focus on streamlining these, maximum benefit can be achieved. A number of steps can be taken to streamline the workflow, and these come under three broad headings of reduced manual processes, increased throughput and improved integration. Dependence on manual processes can be reduced by the automation of liquid handling and extraction, use of barcode reading for worklist generation and implementation of automated data analysis. Throughput can be increased with strategic column and sample management and by analyte multiplexing. Integration can be improved by bi-directional interfacing of the LC/MS-MS system to the laboratory information management system (LIMS) allowing automatic worklist upload and results download. These three strategic areas will be discussed in more detail below.
Reduced manual processes
Unlike the case with immunoassay, samples for LC-MS/MS usually require extraction prior to analysis. Historically this extraction step utilized liquid–liquid extraction or protein precipitation, these being carried out after the addition of internal standard to the calibrators, quality controls and patient samples. All of these steps involved manual pipetting and were very slow and time consuming. Use of an automated liquid-handling platform for the pipetting of samples and addition of internal standard allows some of the steps of liquid–liquid extraction and protein-precipitation methods to be automated. These liquid-handling platforms are available from a number of suppliers including Hamilton and Tecan.
With the advent of 96-well plate technology it became possible to carry out fully automated off-line solid phase extraction (SPE) using platforms such as the Freedom Evo (Tecan) and the Biomek NX (Beckman Coulter). More recently, supported liquid extraction (SLE), which allows solvent extraction to occur on a diatomaceous earth inert support, has also become available in a 96-well plate format. The Extrahera system (Biotage) enables automation of SLE by carrying out all of the pipetting and extraction steps required. In the NWLP laboratory, this system is used for the extraction of patient samples for vitamin D measurement by LC-MS/MS. A sample throughput of up to 50,000 samples per annum is achieved with capacity remaining for additional extractions for use in other LC-MS/MS applications. The system is robust and reliable with good pipetting precision and uses disposable pipette tips, thus avoiding sample carry over. Figure 2 depicts the Tecan Freedom Evo 200 and Biotage Extrahera liquid handlers in use in the NWLP laboratory.
In some manufacturers’ LC-MS/MS systems, on-line sample preparation and extraction is enabled by use of turbo flow or 2D chromatography. On-line protein precipitation and SPE is also now available using the Clinical Laboratory Automated sample preparation Module (CLAM)-2000 (Shimadzu Corporation) [3] and the Rapidfire 365 MS system (Agilent) [4] respectively. These latter examples most closely resemble the immunoassay workflow, whereby samples are introduced into the analytical system without any sample preparation or pre-treatment.
Increased throughput
Increased throughput can be achieved through the use of column and sample managers, allowing multiple assay batches to be queued up for overnight analysis of different LC-MS/MS assays. LC multiplexing enables multiple columns to be coupled to one tandem mass spectrometry system, maximizing the MS detection capability. In this approach, the use of quaternary solvent pumps in the LC enables column switching between different columns using different mobile phases. Finally there is analyte multiplexing, which can use manufacturers’ kits or in-house laboratory developed tests (LDTs). This approach enables multiple analytes to be detected in a single chromatographic separation by the use of multiple reaction monitoring for MS/MS detection. Perkin Elmer and Chromsystems both provide kits enabling the simultaneous measurement of multiple steroid hormones within a single assay panel. In the NWLP laboratory an in-house LDT steroid panel for the simultaneous measurement of androstenedione, 17-hydroxyprogesterone and testosterone has been implemented. This multiplexed assay has replaced the previous stand-alone assays for these analytes, thus increasing throughput and offering faster turnaround time. The assay utilizes off-line SPE using Waters Oasis PRiME HLB 96-well plates and the Tecan Freedom Evo 200 automated liquid handler [5].
Improved integration
Improved integration can be achieved by the use of bi-directional interfacing between the LIMS and the LC-MS/MS instrument software. Nowadays, manufacturers of LC-MS/MS systems offer customer support to allow their systems to be interfaced to the LIMS. One example is the MassLynx LIMS interface (Waters), which enables both worklist download and results upload. The MassLynx LIMS interface is accessed via the LC-MS/MS system software allowing sample worklists, created by barcode scanning of the patient samples, to be imported directly. Following peak integration and analyte quantitation the results are directly transmitted from the LC-MS/MS to the LIMS via an HL7 interface. This avoids the need for manual transcription thus saving a great deal of staff time and eliminating transcription errors.
The ultimate aim of LC-MS/MS integration is to achieve complete integration of LC-MS/MS instruments into the automated workflow of high-throughput routine clinical laboratories. With the recent launch of the Cascadion LC-MS/MS analyser (Thermo Fisher Scientific) this ultimate aim has now been achieved [6]. This analyser offers a complete LC-MS/MS solution including primary blood tube sampling, on-board sample extraction, LIMS connectivity and a random access workflow enabling the provision of a 24/7 service. Traceable manufacturer’s kits are offered for the measurement of a panel of immunosuppressant drugs, testosterone and vitamin D with further assay kits in the development pipeline. The Cascadion analyser is shown in Figure 3.
Summary
LC/MS-MS automation and integration is now a reality, allowing faster sample processing and improved turnaround time, as well as offering increased staff productivity, improved quality and reduced error rate. Staff time is liberated for further service development, allowing the more rapid introduction of validated in-house LDTs into the assay repertoire. Finally there is the possibility of complete analyser integration allowing routine, high-throughput analysis, as is already the standard approach for the common immunoassay platforms. This exciting development will support the more widespread adoption of LC-MS/MS in the routine clinical laboratory by offering complete automation and integration, overcoming the barriers discussed in this article and enabling the inherent advantages of LC/MS-MS in clinical laboratory practice to be more fully realized.
References
1. Jones AM, Honour JW. Unusual results from immunoassays and the role of the clinical endocrinologist. Clin Endocrinol Oxf 2006; 64: 234–244.
2. Zhang YV, Rockwood A. Impact of automation on mass spectrometry. Clin Chim Acta 2015; 450: 298–303.
3. Shimadzu. CLAM-2000. Fully automated sample preparation module for LCMS. (https://www.shimadzu.com/an/lcms/clam/index.html).
4. Jannetto PJ, Langman LJ. High-throughput online solid-phase extraction tandem mass spectrometry: Is it right for your clinical laboratory? Clin Biochem 2016; 49: 1032–1034.
5. Williams EL. LC-MS/MS measurement of serum steroids in the clinical laboratory. Clinical Laboratory International 2017; Sept: 18–20.
6. ThermoFisher Scientific. Cascadion SM Clinical Analyzer (www.thermofisher.com/cascadion).
The author
Emma L. Williams PhD, FRCPath
North West London Pathology, Imperial College Healthcare NHS Trust, London, UK
E-mail: emma.walker15@nhs.net

Anemia in pregnancy is one of the most common medical problems pregnant women encounter in both low and high income countries. It affects some 32 million pregnant women worldwide each year and is characterized by a lack of red blood cells. Women with severe anemia will have a blood count of less than 70 grams of hemoglobin per litre of blood. It is a dangerous condition and if not prevented or treated correctly can lead to maternal death.
Highlighting the danger, an international study published in May this year, shows that women with severe anemia during pregnancy or up to seven days after delivery have double the risk of dying compared to those who don’t suffer from the condition.
Previous studies had suggested that anemia was strongly associated with maternal death, but they were not clear due to the influence of other clinical factors. This study – the largest of its kind – is the first to control factors that can influence the development of anemia in pregnancy (such as blood loss or malaria infection) and which may have skewed the results of previous studies.
The researchers emphasize that clinicians, policy makers and healthcare professionals should now focus their attention on preventing anemia, using a multifaceted approach, and not just hope that iron tablets will solve the problem.
Although anemia is a readily treatable condition, the existing approaches have so far not been able to tackle the problem, say the researchers who published their study in the MAY/ JUNE 2018 issue of The Lancet Global Health.
For the study they looked at World Health Organization data on 312,281 pregnancies in 29 countries around the world. The study results show that, when all known contributing factors are controlled for, the odds of maternal death are doubled in mothers with severe anemia.
Importantly, the relationship between severe anemia and the increased risk of maternal death is seen in different geographical areas and, by using different statistical approaches, the researchers are able to show an independent relationship between severe anemia and maternal death does exist.
Prior to this research, the absence of robust data showing evidence of the relationship between severe anemia and maternal mortality has led to a relatively low prioritization of anemia as an important condition in its own right. This new research will hopefully motivate health policy makers to sharpen their focus on the prevention of anemia during pregnancy when they shape new policy on the condition.
The growth in the use of modern, implantable cardiovascular devices has been accompanied by efforts to have them monitored by professionals at a distance. The principal driver for this has been convenience. However, over recent years, remote monitoring (RM) of cardiovascular devices is emerging not only as an alternative to the clinic, but in some cases as a source for enhancements to quality of care. Several professional societies have issued authoritative guidelines recommending RM for all eligible patients.
Device complexity and data transfer
Formally known as cardiovascular implantable electronic devices (CIEDs), equipment such as pacemakers, cardioverter defibrillators, loop recorders and hemodynamic monitors are technologically complex and equipped with an array of microelectronics, high computational capability and onboard firmware.
In turn, this allows for assessment, storage and remote transfer of a range of data via a transmitter placed in proximity to the patient. Examples of such data include device function, diagnostics and fault codes, to therapy delivery and intra-cardiac hemodynamics, as well as reports on patient clinical status and alerts on cardiovascular events.
Developments in remote monitoring technology
On their part, remote monitoring techniques too have undergone their own evolution – from the original telephonic check-up of pacemaker battery levels and wand-based systems with patient-driven downloads, to current generation products which transmit data through stationary or mobile transmitters by either analogue/digital wired or wireless communication. Once transmitted, medical staff can check the information via a secure Website. Both the type and volume of transmitted data is similar to that obtained from direct interrogation.
Technically, it is important to differentiate between ‘remote interrogation’ and ‘remote monitoring’. The former involves periodic device interrogation performed manually at home by the patient or automatically at predefined points by the monitoring system. RM involves continuous device monitoring, one of whose key features is to trigger transmissions in case of alerts.
Convenience and workflow bottlenecks
Remote monitoring eliminates the need for routine, periodic visits to a clinic after CIED implantation. Most international guidelines specify that patients fitted with CIEDs should be followed up routinely, with the frequency depending on the device type and model – for instance, at Months 1 and 3 for implantable cardioverter defibrillators (ICDs). Key checks include those on battery, lead impedance, sensing amplitude, pacing threshold and arrhythmic events.
One of the most perceptible advantages of RM is of course convenience. Before it became available, patients with CIEDs had to visit clinics for periodic checks. This was a problem for several categories of patients – above all, those living in rural areas and those needing to be escorted by families due to frailty. These factors assume additional significance since the number of CIED patients has not only been increasing due to maturing technology and expanded indications, but also because an ageing society means that more people are in need of the devices. As a result, it is becoming ever-tougher to make appointments for CIED checks, and many patients who do not have RM can spend several hours waiting at a hospital for their turn.
Remote monitoring eliminates such bottlenecks and choke points. Analysis of RM data before a patient visit can shorten the time required for direct interrogation and intervention, especially should a need arise to determine the cause and management of a problem. If such a problem is only detected during a clinic visit, a patient would have to wait for the results to be verified, while the problem is detected, analysed and resolved.
According to some estimates, time required by physician to review RM data is approximately 10 minutes compared to a half-hour to complete CIED follow-up visits in a clinic.
Apart from routine transmission, special real-time protocols exist in RM for alerts, such as data anomalies, inappropriate therapy or other abnormalities. In such cases, the transmitter is usually linked to a central secure server to back up or distribute the results to a larger number of experts for further analysis and opinion.
RM data essentials
Typical data reported by RM include arrhythmic events (real-time intra-cardiac electrocardiogram, to determine if the event is supra-ventricular or ventricular), premature ventricular contractions (based on PVC frequency recording), atrial fibrillation (especially promising for patients with no prior history of AF, to allow rapid anticoagulant drug administration and prevent stroke), non-sustained VT (although this is mainly considered for ICD or CRT-D patients, rather than those with pacemakers) and VT/VF (to enable a therapy decision and whether it can be managed at home).
The Finnish ICD study
Meanwhile, rigorous observational and randomized studies have demonstrated a variety of clinical benefits, along with a high degree of patient satisfaction as well as cost effectiveness.
One of the first major studies on remote monitoring of ICDs was carried out in 2005-2006 at the Oulu University Hospital, Finland. The system consisted of a portable patient monitor, a secure database and website, at which clinicians could view and analyse data.
The study’s goal was to provide comprehensive information on the safety, ease of use, satisfaction and data acceptance by both clinicians and patients, and the cost-effectiveness of remote monitoring in a location characterized by long travel distances to the clinic.
The outcomes were satisfactory.
There were, first of all, no device-related adverse events.
80% of the remote-monitoring sessions were performed by the patients without any assistance. Indeed, ease of use and satisfaction by both patients and clinicians made an especially strong case. Most patients found the instructions ‘clear’ or ‘very clear’, with monitor set up ‘easy’ or ‘very easy’. What was equally significant was the lack of any major difference in patient feedback from the first test, at 3 and 6 months, and even during unscheduled visits.
On their side, clinicians too drew similar conclusions on ease of use and satisfaction, with the majority finding data comparable to traditional device interrogation. Just two of 137 physicians felt an in-office visit would have provided more detailed information on device function, as it was not possible to measure the pacing threshold remotely.
Early detection of clinical events
Since then, other studies have reconfirmed the immense promise of RM.
In 2010 ‘Circulation’ published results of a trial on automated remote monitoring of implantable cardioverter-defibrillator called TRUST (Lumos-T Safely Reduces Routine Office Device Follow-up).
This study, on 1,339 patients, confirmed that the burden of visiting a clinic was greatly reduced by using RM, and that it saved valuable time and resources. The study found that in-hospital evaluation numbers dropped by 45% without affecting morbidity.
The TRUST trial also established that RM facilitated early detection of clinical events, in some cases dramatically. For example, the median period from onset to physician evaluation of combined first atrial fibrillation (AF), ventricular tachycardia (VT), and ventricular fibrillation (VF) events with RM was 1 day. By comparison, conventional care reported a median period of 35.5 days. System-related problems (such as lead out-of-range impedance) occurred over four times less frequently with the RM group, although the incidence in either setting was far too low to make meaningful comparisons.
Wireless RM and cardiac hospitalization stays
The utility of wireless remote monitoring with automatic clinician alerts was the subject of another trial called CONNECT (Clinical Evaluation of Remote Notification to Reduce Time to Clinical Decision). This multicentre, prospective, randomized study of almost 2,000 patients with high-energy CIEDs lasted for 15 months. Its results were published in ‘The Journal of the American College of Cardiology’ in 2011, and reported a decrease in mean length of stay per cardiovascular hospitalization visit from 4 days in an in-office setting to 3.3 days with RM. The CONNECT study also found a dramatic reduction in the median time to a clinical decision in response to events, from 22 days at a clinic to 4.6 days using RM.
Other benefits of RM
RM has also established some other dramatic benefits. In 2013, ‘The European Heart Journal’ reported on ECOST, a randomized study on remote follow-up of ICDs. ECOST found that patients with RM had a 52% reduction in inappropriate shocks, fewer hospital admissions after such events and 76% fewer capacitor charges, leading to longer battery life.
In December 2014, a report in ‘The Journal of Arrhythmia’ noted that in prophylactic ICD recipients, the recommended 3-month in-office follow-up interval could be extended to 12 months with automatic daily RM, and that this reduced the ICD follow-up burden over a 27-month period after implantation. The 12-month interval resulted in more than halving the total number of in-clinic ICD follow-ups. In addition, no significant difference was found between the two groups (3-month in-clinic follow-up versus 12-month RM) in mortality, hospitalization rate, or hospitalization length over the observation period.
Mortality reduction with RM
Indeed, some experts propose that RM may reduce mortality in patients with CIEDs.
One study called ALTITUDE assessed long-term outcomes after ICD and cardiac resynchronization therapy (CRT) implantation and the impact of RM on almost 70,000 ICD and CRT-plus-defibrillator (CRT-D) patients. It found that one- and 5-year survival rates were 50% higher in comparison to about 115,000 patients who received CIED follow-up in office visits.
The future: patients generally satisfied with RM
As technology continues to evolve, both new possibilities and questions are emerging. In the years to come, remote monitoring holds forth considerable promise for future research, given that massive amounts of data have already been collected from patients.
In spite of some typical first-mover tech concerns, RM has proven to be easy to use and well accepted, even by the elderly people and patients with low education levels. There are some patients, however, who do not accept RM. This is mainly due to suspicions about technology and the risk of losing human contact with nurses and physicians. In such cases, patient education is critical.
The other challenge involves keeping track of a flood of data and alerts from a fast-growing pool of patients. As described previously, RM detects cardiovascular events much earlier than conventional follow-up. As a result, it is becoming essential to assess whether this translates into clinical benefits for patients, or whether earlier detection of events due to RM excessively increases clinic visits; the latter might well reduce clinical benefits.
On their part, patients continue to be satisfied with RM in terms of ease of use. One Italian study at San Filippo Neri Hospital in Rome has reported a more favourable change in quality of life over a 16-month period in RM patients, compared to those lacking access to RM. Benefits which have been specifically highlighted include the patients’ peace of mind, psychological well-being, and safety.

Smartphones are turning out to be an exciting weapon against the scourge of cardiovascular disease, which is considered by the World Health Organization (WHO) to be the most common cause of death worldwide.
Reasons for such a development are varied. Smartphones bristle with sensors like cameras and accelerometers which can be used for making, storing and transmitting diagnostic measurements. Smartphones are also small, mobile and capable of being paired with wearable devices such as wristbands, watches, skin patches etc.
Real-time and continuous measurement
The concept of always-on continuity, enabled by smartphones, makes sense in several cardiovascular health-related contexts. To date, most authoritative studies in this field are based on questionnaires, and focused on variables like diet, exercise, sleep etc. They have also relied almost wholly on participant recall.
By contrast, the sensors in mobile smartphones allow for real-time and continuous measurement of a range of factors. This can make a major difference.
For instance, high blood pressure (hypertension) is known to be a leading cause of strokes and heart attacks. However, blood pressure is very difficult to measure precisely. It can vary widely over just one day, and increase if one simply dangles one’s feet off a table, or for that matter becomes stressed by the exam itself. In this case, a wearable which monitors blood pressure through the day and night, and provides an average over time to compare with those from previous days or weeks, has clear advantages over the spot metric offered by blood pressure measurement at a physician’s clinic.
Applications in atrial fibrillation
Elsewhere, smartphone apps are now targeting the diagnosis of irregular heart rhythms, which can indicate atrial fibrillation (AF), another major cardiovascular risk. Such irregularities need not be symptomatic, but can be all the more dangerous because of that.
In 2014, the US Food and Drug Administration (FDA) approved the AliveCor Heart Monitor, which consists of a smartphone app plus a phone case fitted on its back with special sensors. Touching the sensors allows visualization of cardiac electrical activity on the phone screen.
Currently, a host of other smartphone apps alert users about potential AF without requiring any special sensor-equipped case. Though yet to be cleared by the FDA, reports suggest they might be similar in accuracy to AliveCor.
Migration from fitness to the medical
Another approach to arrhythmia has been taken by the Media Lab at the Massachusetts Institute of Technology (MIT). The latter’s Cardiio spin-off also illustrates the potential for migrating smartphone apps from fitness monitoring to the medical. In 2012, Cardiio launched an eponymous fitness app to measure heart rate based on facial light reflection, given that a beating heart pumps and increases blood volume in the vessels. On its part, blood hemoglobin absorbs light, and this decreases the amount of light reflected by the skin. Though such tiny changes in reflection are invisible to the human eye, they can be sensed by smartphone cameras and interpreted by apps.
Cardiio recently deployed its light-reflection system in another app, which detects the irregular heartbeat patterns of atrial fibrillation.
An electrocardiogram (ECG), which involves the attachment of electrodes to the chest to measure electrical impulses in a heartbeat and detect irregularities, remains the standard for AF-detection. However, as in the case of the blood pressure variations mentioned above, clinicians are aware that an ECG might not pick up an AF, should the heart rhythm irregularity be sporadic. Indeed, in some cases, irregularities are discovered only after patients suffer a stroke. One of the most common of these is known as paroxysmal AF, which causes spontaneous irregular heartbeats that are not straightforward to diagnose.
Supplementing traditions, new frontiers
In general, no one believes that smartphones will replace diagnosis by traditional medical devices. However, they have begun to supplement the latter, and are expected to continue doing so. Such a process is taking smartphones into ever-newer frontiers.
For example, engineers at the California Institute of Technology (Caltech) have demonstrated a smartphone app which measures ‘left ventricular ejection fraction’ (LVEF). LVEF is the volume of blood pumped by the heart per beat as the arteries expand and contract, and is one of the principal measures of heart health. It is typically assessed by ultrasound, which can take hours and be performed only by technicians.
The Caltech app requires patients to hold a smartphone camera against the carotid artery in their neck. This feeds directly into the heart and provides especially accurate information. The procedure, which lasts under two minutes, involves the camera measuring the expansion and contraction of the carotid artery’s walls. An algorithm in the app uses this data to calculate blood flow from the heart. According to some reports, the app provides LVEF data which is as accurate as an ultrasound.
Many industry experts foresee that next generation wearables will have ECG and pulse oximetry capabilities, with some going as far as predicting that wearables, supported by sensors embedded discretely in clothing, could be used for continuous blood glucose and blood pressure monitoring.
Part of wider mHealth drive
As smartphones begin to be seen as a strategy to fight cardiovascular disease, many manufacturers and app developers have sought to commercially capitalize on the wider mobile personal health (mHealth) movement. Indeed, it is now becoming accepted that mobile devices and apps can provide data to make meaningful and informed clinical decisions.
For some cardiovascular conditions, mHealth is also seen as enhancing the ability for pre-emptive intervention by giving patients more accessible diagnostic tools and information.
Indeed, CVD prevention represents an ideal zone for propagating and popularizing mHealth. Cost‐efficient and scalable approaches can yield large scale insights into behaviours shaping/adversely impacting on cardiovascular health. Such solutions, in turn, can provide the raison d’etre for interventions which seek to change risky behaviour.
To make this work in the long term, however, providers, payers and professional societies concerned with cardiovascular health need to closely partner with mHealth developers. So too should regulators, especially given the emergence of a growing body of evidence about the benefits of smartphone-driven mHealth – not least in areas such as cardiovascular health.
Universities join industry in research
Until now, the gap in conclusive evidence has largely been on the clinical side, and there have been calls for more research to see how viable – and valuable – such solutions really are.
In January 2017, the authoritative ‘Journal of the American Medical Association’ published the results of a smartphone-centric cardiovascular study in the US, with physical activity patterns tracked and identified through cluster analysis and correlated with self-reported disease. The study found that a pattern of lower overall activity with more frequent transitions between active and inactive states was associated with the prevalence of equivalent self-reported cardiovascular disease as a function of higher overall activity with fewer transitions.
The JAMA study also drew several other conclusions. The first was confirmation of the existence of a sufficiently large smartphone-using population, who could be engaged to demonstrate cardiovascular health status using smartphones. Secondly, it showed that large-scale, real-time data could be gathered from mobile devices, stored, transferred and shared securely. The authors also noted that more data than any previous collected about the standard six-minute walk test could be generated in weeks.
Industry is enthusiastically upporting these efforts. The Apple Watch app Cardiogram, for example, has presented results saying that it could diagnose atrial fibrillation with 97 percent accuracy. Cardiogram had collaborated with the University of California San Francisco as part of Heart eHealth, the largest study to date on mHealth and heart disease. Apple recently announced it would be partnering with Stanford University researchers to run a study targeted at investigating AF.
Europe launches apps aimed at patients and professionals
In Europe, the European Society of Cardiology (ESC) has funded the creation of two AF apps targeted at patients, and at healthcare professionals.
The patient app provides education on AF, including sections on pathology, symptoms, prognosis, associated co-morbidities, management strategies and practical self-care tips. It is also designed to present information on individual stroke risk and provide a personal health record and symptom diary. On their part, patients fill in sections about their relevant health histories, which can facilitate consultation when shared with their healthcare professionals.
The professional app is designed as an interactive management tool incorporating new ESC Practice Guidelines on AF, and allows both conventional viewing of guideline text and recommendations, as well as interactive treatment algorithms. It is also aimed at improving consultation efficiency, via the provision of a patient register, pre-filled with data supplied by the patient app mentioned above.
Need for caution remains
In spite of all the buzz around smartphones and cardiovascular health, several experts have also been urging caution.
Major issues include a lack of representativeness. The bulk of smartphone users, not least those willing to experiment with new apps, are young, while cardiovascular disease risks rise in older age groups. In the US, for example, only 12% of adults aged over 65 years are estimated to own a smartphone.
Some studies in Europe have found such trends to be reversing. For example, a survey by consultants Deloitte in the UK last year indicates that 71% of 55-to-75 year olds now own an app-capable handset, and this age group has seen a faster adoption rate than any other over the past five years. However, members of the demographic tended to use their smartphones less than younger people.
Finally, younger users can also be fickle, with a steep drop-off in engagement over time. One survey found that only 80% of consumers continued to use their wearables regularly after three months. Such factors can produce major risks for data integrity in a study.
The limits of mass consumer technology
Another problem is technology. In spite of dramatic progress in recent years, an Apple Watch is easy to cheat.
Accuracy is another drawback. One smartphone app to measure blood pressure required users to place a smartphone against their chest and a finger over the camera. However, it was discovered to have missed high blood pressure in as many as eight of 10 patients. This was also the problem with a phone case which sought to measure blood pressure at the fingertip, but studies were inconclusive about whether the case was good enough for use in a home environment.
Healthcare professionals point to some more serious limitations. Devices checking heart rates infer rhythms from the pulse, and it is possible to have a normal pulse with an abnormal heart rhythm.

Two studies on information technology and patient safety were released in the US in April 2018.
The first, by ECRI Institute and its Partnership for Health IT Patient Safety stakeholder collaborative, takes a searching look at the hidden risks of healthcare IT (information technology) systems.
The second report, by Pew Charitable Trusts, focuses on electronic health records (EHRs), and is based on its long-standing view that in spite of more than 30 billion dollars (£25 billion) of federal health IT investment over the past decade, the transition from paper to electronic records has yet to reach its potential to enhance healthcare coordination and improve patient safety.
Both studies call for a much greater degree of proactivity to anticipate problems before they run out of control. Interestingly, there also seem to be several parallels in their respective analyses of the challenges.
A broad-based look at patient safety
One of the first priorities for healthcare organizations is to tie health IT into existing patient safety initiatives. The challenges that exist whenever older systems are updated or replaced, or integrated with successor technologies, can ideally become learning opportunities. However, this requires the organization to have a collaborative management culture that makes initiatives such as IT safety and other best practices part of their daily workflow.
Both the ECRI and Pew are emphatic about the need for collaboration. ECRI lays down specific recommendations on obtaining feedback from stakeholders (patients, payers, cybersecurity experts, regulators, providers and others). The Pew report also maintains that collaboratively gathering inputs from across the healthcare stakeholder spectrum is critical to improve patient care and reduce provider burden in the context of EHR use.
Tip of the iceberg
The ECRI Safe Practice Recommendations begin with an ominous warning – that the known universe of IT-related safety problems are likely to be just the tip of the proverbial iceberg. The net risk from such issues is that a variety of bugs are lurking beneath the surface, and, in the ECRI’s view, pose permanent dangers to patients. Such risks, in turn, are compounded by the sharp growth in recent years of ransomware and other cybersecurity threats which seek to exploit loopholes in codes. For ECRI, this is a key reason why both providers and vendors need to make health IT safety an integral part of their overall patient safety program.
The ‘over’-customization quandary
In general, the roots of healthcare IT problems stretch back to the 1980s and 1990s when demands for customization led to ad-hoc rewriting of legacy programs, so as to avoid loss of functionalities. So-called patches, as part of platform updates, also sought to retain some of these functionalities, many of which had been proven – or otherwise become indispensable – over the years. During this process, poor documentation of code changes was commonplace. In addition, since legacy systems faced many problems communicating with one another across their proverbial silos, layers of integrative middleware were added in sequence until they became cluttered and unmanageable.
Many such concerns are reflected by Pew. Over customization, auto-refresh mix-ups and unclear default settings with EHRs, as well as alert fatigue, can all result in patient harm.
An earlier Pew report in December 2017 had explained that safety problems could be caused by the very design of an EHR system (e.g. complex interfaces and guidance terminology) or by its customization during implementation and adaptation. Like the middleware in an IT system, Pew explains that an EHR “interface that is cluttered may cause confusion or an inability to locate key information, whereas an overly bare display may force the clinician to search for information in multiple places.”
Indeed, some of the reasons for risky over-customization of EHRs directly reflect those made during program rewrites to legacy IT systems in the 1980s and 1990s.
As the Pew study observes, healthcare facilities often work with vendors to customize certain aspects of their EHR system which fit their workflow, for example by displaying data which is critical for specific clinicians at a particular facility. However, it warns, such customizations “may not have undergone rigorous testing and could lead to unintended safety consequences.”
Specific risks with EHRs
The Pew report highlights a range of specific risks. One of the most commonplace may consist of mix-ups in auto-refresh of patient lists when EHRs revert to the default view. In such cases, providers can inadvertently make medical decisions based on another patient, rather than the one being treated, if they do not realize the system has just refreshed a particular list.
Default EHR settings are also seen as a specific danger for medication dosages. Healthcare providers may think they are ordering a fixed dose of a particular drug, while what they enter instead “is multiplied by the patient’s weight, potentially contributing to overdoses,” Pew notes.
Yet another problem consists of incomplete laboratory results, which can result in erroneous medical decisions since a provider lacks complete information on a particular patient. In effect, physicians may fail to realize that not all lab results are displayed on a screen, or that results may have been delayed – among other reasons, because samples might still be undergoing testing.
In its recommendation to integrate health IT safety into a broader safety program, the ECRI report also pointed explicitly to the rise in duplicate medication errors after a new EHR implementation. Contributing factors include the design of the EHR as well as the occurrence of task-related changes (such as multiple persons entering orders for the same patient at the same time).
Other EHR-related problems mentioned as cases by ECRI included data entry of a pediatric patient’s weight in pounds rather than kilograms – followed by erroneous medication dose, incorrect alert responses due to the simultaneous opening of multiple patient charts, the inability to account for problems such as a pending swallow evaluation before a dietary order, or an allergy to eggs which contraindicate propofol.
Some of the most frequent EHR problems concerned mix-ups of patients, in one instance due to two having the same name !
New safety approaches: collaboration and workflow integration
Beyond EHRs, as the hitherto-unknown problems in the health IT iceberg become more apparent with time, users are advised by the ECRI to collaborate in order to integrate and embed new safety practices into their daily workflow. Suggestions include the provision of inc entives for actively working together on safety-related efforts, and to learn and share analysis of near-misses and other hazards, as well as workaround strategies.
Pew too had stressed the importance of collaboration for improved EHR use, in its December 2017 report. One way towards this is to bring stakeholders together to share data on patient safety incidents and do this in a “nonpunitive environment.” After this, stakeholders can be encouraged to “develop solutions for common and significant usability issues.”
Pew also suggests that safety tests on functionality and usability are conducted by entities throughout the entire EHR life-cycle – from development and after implementation. Such a process should bring together developers, IT professionals, clinicians, nurses and pharmacists – in essence, every one using the EHR system.
Pew cautions that one specific area for attention is alert fatigue (due to too many unnecessary or false alerts). This can result in genuine life-saving warnings being missed. One concrete means to avoid such conundrums is by designing EHR systems to specifically verify and red flag certain potential problems (e.g. dangerous drug interactions with different medications).
The need for encouraging a collaborative culture to enhance healthcare IT safety has also been identified in Europe. In 2015, a team led by Solvejg Kristensen at Denmark’s Aalborg University studied the association of quality management systems with teamwork and safety from seven European countries. Although they found different approaches to quality management systems and to perceptions of teamwork and safety climate, they noted the importance of organizations investing in leadership, time, capital and technical expertise to attain continuous quality improvement and enhance patient safety.
Indeed, at whichever facet of the healthcare technology spectrum one looks at, proactive, meaningfully structured collaboration may be the only way to achieve a unified vision of safe health IT and a wider culture of safety in the health enterprise.
As healthcare IT becomes increasingly pervasive, such concerns are bound to demand increasing attention.
The National Patient Safety Foundation and IHI
Many of these issues – in terms of both challenge and response – were the subject of a set of eight recommendations made in 2015 in a report from the National Patient Safety Foundation (NPSF) in the US to ensure “that technology is safe and optimized to improve patient safety”. The recommendations are as follows:
European initiatives
In 2016, the NPSF added that it was also important to make health IT-related patient safety an organizational priority by securing management commitment, and to develop an environment which was “conducive to detecting, fixing and learning from system vulnerabilities.”
The NPSF was merged with the Institute for Healthcare Improvement (IHI) last year, and some of its initiatives are likely to be transferred to Europe via the IHI Health Improvement Alliance Europe (HIAE), which aims to improve work processes and create new delivery models relevant to European health systems. The HIAE has already established connections with professional societies in several countries, including Britain, Denmark and Belgium.
One good example of HIAE efforts is the The Platform for Continuous Improvement of Quality of Care and Patient Safety (PAQS), a Belgium-based initiative which aims to consolidate relationships between various stakeholders in healthcare in order to work together, in a consistent and cohesive manner.
Other facets of IHI which are expected to make a mark in Europe include the so-called Open School Online Courses. Several of these are directly concerned with IT-focused elements of patient safety and the need to build a culture of safety in a health organization.

MEDICAL FAIR ASIA 2018, is set to continue its growth path with its 12th edition. An expected 1,000 exhibitors from 50 countries and 20 national pavilions will grace the exhibition to be held in Singapore from 29th to 31st August. Visitors will get to source from a comprehensive range of more than 5,000 products ranging from digital health technology, electromedical equipment, rehabilitation supplies to consumables.
There will be a total of 20 National Pavilions and Country Groups, this edition will see debut group participations from Belgium, Brazil, the Netherlands, Iran, Denmark, European Union Business Avenue, Russia, Spain and Qatar, adding to the internationality of the exhibition.
Inaugural Community Care Pavilion
On the show floor, visitors can also expect to see products relating to the current healthcare trends and needs of the Asian region. The debuting Community Care Pavilion, with its keen focus on geriatrics and digital health technology seeks to address the healthcare needs of both the ageing population and the region’s remote population by bringing healthcare beyond traditional healthcare institutions and into the community. Exhibitors have already arranged for product launches to take place during the 3-day period. France Bed Co Ltd will be showcasing their unique powered turning bed. It features an automatic turning support function that prevents users from bed sores. Xiaoniu Health Co Ltd will be unveiling their intelligent sleep machine that can perform both CPAP and AutoCPAP to sleep apnea patients.
Another first on the show floor is the inaugural Start-Up Park. Providing a platform for young and exciting start-ups, the exhibits will feature products that could transform the market in the near future including the latest innovations in big data, and IoT. Australian start-up Rapid Response Revival Research will unveil a prototype of their phone case defibrillator, CellAED, the world’s smallest, lightest and first truly mobile AED (Automatic External Defibrillator) for the very first time.
Conferences and forums
Back by popular demand, the exhibition will play host to the second edition of the MEDICINE + SPORTS Conference. This benchmark event for sports medicine will discuss topics ranging from digital innovations in sports and healthcare, exercise medicine to tailored exercise programmes for patients and athletes. A stellar lineup of speakers including experts Dr. Paul Gastin, Director for the Centre for Sport Research at Deakin University, Mr. Christian Stammel, CEO of WT | Wearable Technologies and Prof. James S. Skinner, Professor Emeritus in the Department of Kinesiology, Indiana University, have been confirmed.
With Start-Ups and SMEs deepening their presence in global business, the exhibition will also host the Medtech SME Workshop. Organized by the first and only regional medical technology association, Asia Pacific Medical Technology Association (APACMed), the workshop will provide small businesses with concise knowledge on clinical trials, product validation, patent laws and many others. Through this workshop, Medtech start-ups and SMEs can learn to navigate processes to develop cost-effective solutions to meet the region’s healthcare needs.
In line with the highlight on Community Care, the exhibition will also feature the first-ever Paradigm Shifts in Healthcare seminar from 30th to 31st August. Leading speakers will discuss the evolution of the healthcare industry while attendees learn how to overcome future challenges as healthcare goes beyond hospitals to the community.
Supported by the Robotic Surgery Society of Singapore, the Medical Innovation & Technology Forum will focus on robotic surgery and discuss how patients evolve from passive healthcare recipients to active value-seekers, encouraging healthcare providers to tap into the latest technological advances to provide more efficient treatment options.
www.medicalfair-thailand.com

Prins Hendrikstraat 1
5611HH Eindhoven
The Netherlands
info@interhospi.com
PanGlobal Media IS not responsible for any error or omission that might occur in the electronic display of product or company data.
