



Improving cleaning practices to reduce the transmission of nosocomial infections is considered a priority in our hospitals. However a recent robust study demonstrates that around 40% of these infections are catheter-associated urinary tract infections (UTIs), and few hospitals surveyed are combating this problem aggressively. The organisms most frequently involved are normal inhabitants of the bowel, such as Escherichia coli. Pathogens form biofilms on the extraluminal and to a lesser extent intraluminal catheter surfaces where they are protected from both the effects of antimicrobials and the immune response of the host. A recent study from Canada reported that the infection rate from indwelling urinary catheters was around 5 out of 100 patients per day. Another robust study found that between 10% and 27% of catherised patients had bacteria in their urine within five days of the procedure being carried out. Comprehensive studies of elderly hospitalised patients have found that those with indwelling urinary catheters have significantly longer stays and are more likely to die in hospital. While symptomatic UTIs are the most frequent complication of catherisation, chronic pyelonephritis has been found at autopsy in approximately one third of patients who had indwelling urinary catheters, and their long-term use has been associated with bladder fibrosis and an increased risk of bladder cancer.
Of course the insertion of a urinary catheter can be a medical necessity, and in this case careful attention should be given to aseptic insertion techniques as well as the choice of device [see this issue of IHE, page 6]. However it would be prudent, given the increased morbidity and mortality associated with the procedure, to question, prior to each insertion, whether it is really necessary. A concerted effort should also be made to limit the duration of catheterisation should it be medically indicated. Yet a multi-centre study in the US found that in around 30% of cases the attending physician did not know if his/her hospitalised patient had an indwelling urinary catheter or not. In 31% of cases the catheters were found to be unnecessary.
A plethora of other studies has shown that, particularly in elderly patients, indwelling catheters are frequently used for the benefit of over-worked healthcare personnel rather than because their use is medically indicated. The most common reasons reported for unnecessary catheterisation are patient incontinence, cognitive impairment and impaired mobility.
It is indeed apalling to think that patients
Multiple strategies have been deployed to reduce catheter associated urinary tract infections. These include employing correct hand-washing procedures, avoiding breakages in the urinary collection system and taking measures to prevent commensal bacteria from the patient contaminating the catheter. As well as changes in clinical practice, we need to be mindful of the potential technological and equipment solutions. This article highlights the potential use of silver-alloy urinary catheters to reduce catheter associated urinary tract infections.
by Michelle Beattie
Catheter associated urinary tract infections are often accompanied by an increased period of hospitalisation and morbidity, resulting in poor outcomes for patients as well as their families, and significant economic costs to service providers. Despite the high risk of infection and other potential complications, urinary catheters have many beneficial uses in healthcare including diagnostic, prophylactic and therapeutic uses. Regardless of whether the urinary catheter is used for therapeutic or diagnostic purposes, catheters should only be inserted when deemed absolutely necessary, due to their association with significant morbidity and mortality [1].
Catheterisation and sources of infection
As urinary catheterisation involves the insertion of a catheter into the bladder via the urethra, the patient is at a higher risk of infection, as essentially the body treats the presence of a catheter as a foreign body. The body

Recent studies have demonstrated that several major nosocomial pathogens are shed by patients and contaminate hospital surfaces at concentrations sufficient for transmission, survive for extended periods, persist despite attempts to disinfect or remove them, and can be transferred to the hands of healthcare workers. Evidence is accumulating that contaminated surfaces make an important contribution to the epidemic and endemic transmission of Clostridium difficile, vancomycin-resistant enterococci, MRSA, Acinetobacter baumannii, Pseudomonas aeruginosa and norovirus, and that improved environmental decontamination contributes to the control of outbreaks.
by Dr Jonathan A. Otter
Hospital patients shed pathogens into their surrounding environments but there is debate over the importance of the resulting surface contamination as a source for subsequent transmission. Several studies in the early 1980s suggested that the hospital environment contributed negligibly to endemic transmission. Recently, however, there has been a reassessment of the role of contaminated surfaces in the transmission of nosocomial pathogens.
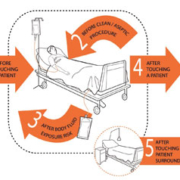
Pathogen transfer from an affected patient to a susceptible host occurs most commonly via the hands of healthcare workers (HCWs) but contaminated objects, surfaces and air can be either directly or indirectly involved in transmission [Figure 1]. Here we review evidence that nosocomial pathogens are shed by patients and can contaminate hospital surfaces at concentrations sufficient for transmission, can survive for extended periods, can persist despite attempts to disinfect or remove them and can be transferred to the hands of healthcare workers (HCWs) [1]. We also review evidence that improved environmental hygiene can help to bring outbreaks under control and reduce endemic nosocomial transmission.
Pathogens are shed into the hospital environment
Several important pathogens including Clostridium difficile, methicillin-resistant Staphylococcus aureus (MRSA), vancomycin-resistant enterococci (VRE), Acinetobacter baumannii and norovirus can be shed by patients into the hospital environment and share the ability to survive on dry surfaces for extended periods. Under certain conditions, C. difficile spores, VRE, MRSA and Acinetobacter spp. can survive for 4-5 months or more on dry surfaces and norovirus can survive for a week or more [2]. Wide variation in the reported frequency of environmental contamination can be explained by several factors, including the degree of shedding by the patient, the culturability of the organism, the sampling methodology and the ease of contamination (or difficulty of cleaning) of the particular environment. Methodological differences in sample collection and culture make comparisons between studies difficult and in some cases the true level of environmental contamination may be underestimated.
Patients are the prime source of contamination, so surfaces in the vicinity of patients that are touched frequently by healthcare workers and patients, termed
Patients are at risk of infection from the numerous types of pathogens that can survive in hospitals. The cleaning process could have a huge impact on this risk if it is aimed at the most frequently contaminated sites, removes or kills viable organisms and is carried out sufficiently frequently to inhibit accumulation of pathogens. Whilst there are an increasing number of products on the market to facilitate the cleaning process, evidence of their efficacy is needed. Frequent detergent-based cleaning also requires urgent appraisal in order to compare alternatives for cleaning hospitals.
by Dr Stephanie J. Dancer
More evidence is accumulating for the role of cleaning in controlling infection in hospitals. There are a variety of hardy hospital pathogens such as meticillin-resistant Staphylococcus aureus (MRSA), vancomycin-resistant enterococci (VRE), norovirus, Acinetobacter and Clostridium difficile, all of which can persist in healthcare environments for considerable lengths of time. Basic cleaning can help in the control of these pathogens, usually as part of an overall package in response to an outbreak, but there is also a role for enhanced cleaning in the non-outbreak situation. Organisms on hand-touch sites in hospitals are thought to provide the most important risk for transmission because hand contact with a contaminated site could deliver a pathogen to a patient. However, current cleaning regimens do not necessarily target high-risk reservoirs and there remains confusion between nursing and domestic personnel over allocation of cleaning responsibilities. Whilst there is little evidence for the most effective cleaning frequencies, some sites do not receive the cleaning attention that they deserve. Thus, cleaning practices should be tailored to clinical risk, as well as reflect the wide-ranging surfaces, equipment and building designs in today
Hand hygiene is a crucial part of patient safety in healthcare settings. Hand hygiene promotion using a multimodal strategy incorporating alcohol-based handrub is now the standard of care. A wealth of information and practical tools are available through the World Health Organisation
Prins Hendrikstraat 1
5611HH Eindhoven
The Netherlands
info@interhospi.com
PanGlobal Media IS not responsible for any error or omission that might occur in the electronic display of product or company data.
